Provincial Laboratory for Public Health (Microbiology)(ProvLab), Calgary, Alberta, Canada.
Global Health. 2010 Nov 1;6:20. doi: 10.1186/1744-8603-6-20.
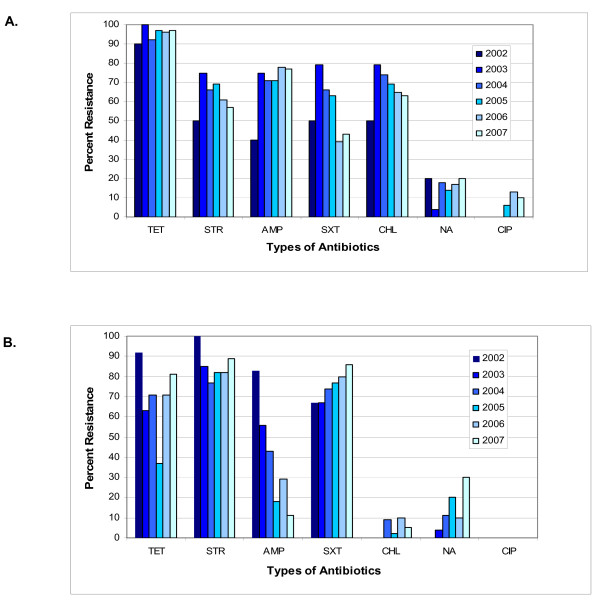
Between 2002 and 2007, travel related cases of Shigella sonnei and S. flexneri in Alberta, Canada were acquired from Central America, the Indian subcontinent and North America. Of this group, resistance to ciprofloxacin and nalidixic acid was identified in isolates from patients who had travelled to the Indian subcontinent. This study provides a Canadian perspective to a growing body of literature linking ciprofloxacin and nalidixic acid resistance to travel to the Indian subcontinent.Shigella is a common cause of diarrheal illness in North America with a rate of 2.0 per 100,000 in Canada 1 and a rate of 3.2 per 100,000 in the United States 23. Imported cases of Shigella infections have been reported in developed countries following travel to a foreign or developing country 45 and may be impacted by factors including socio-economic factors 6, food distribution networks 5 and microbiologic factors 7. Across multiple geographic regions, high rates of antimicrobial resistance to multiple agents (e.g. sulfonamides, tetracycline, chloramphenicol, ampicillin, and trimethoprim-sulfamethoxazole) have limited the choices for empiric antimicrobial therapy required to manage Shigella infections and reduce fecal excretion of the bacteria 8910 with descriptions of shifting species dominance and changes in antimicrobial susceptibility 1011. Generally, Shigella flexneri and Shigella sonnei are the dominant species and are heavily impacted by changes in antimicrobial susceptibility 1213.This study identifies the global regions associated with travel-related cases of S. flexneri and S. sonnei in Alberta, Canada and compares antibiotic resistance patterns of these isolates for 2002 to 2007 inclusive.Specimens collected 2002-2007 (inclusive) from S. flexneri and S. sonnei infections in Alberta, Canada were included for study. Data collected at time of specimen submission included: date of specimen collection, outbreak association if present, travel history and antibiogram (data source-ProvLab Information Systems; Communicable Disease Report at Alberta Health and Wellness). Outbreaks were defined by public health officials as ≥ 2 epidemiologically related cases. Each outbreak was assigned a unique incident number. Repeat isolates received within six months of original case infections were excluded. Only one representative case for each outbreak was included, unless the isolates had different antibiotic susceptibility patterns. Based on travel history the origin of an isolate was grouped into corresponding regions and continents. Regions included in the study represented major travel destinations for individuals living in Canada. Domestic exposures were defined as "travel within North America."
2002 年至 2007 年间,加拿大艾伯塔省的旅行者感染志贺氏菌(包括宋内志贺氏菌和福氏志贺氏菌)病例均来自中美洲、南亚和北美地区。该组患者中,来自南亚旅行者的志贺氏菌分离株对环丙沙星和萘啶酸耐药。本研究从加拿大的角度为越来越多的文献提供了依据,这些文献将环丙沙星和萘啶酸耐药与前往南亚旅行联系起来。志贺氏菌是北美地区常见的腹泻病病原体,在加拿大的发病率为每 10 万人 2.0 例,在美国为每 10 万人 3.2 例 1,2。在发达国家,旅行者在国外或发展中国家旅行后会报告志贺氏菌感染病例 3,4,并且可能受到社会经济因素 6、食品分销网络 5 和微生物因素 7 的影响。在多个地理区域,多种药物(如磺胺类药物、四环素、氯霉素、氨苄西林和复方磺胺甲噁唑)的耐药率较高,限制了管理志贺氏菌感染所需的经验性抗菌治疗药物的选择,并减少了细菌的粪便排泄 8910,同时描述了物种优势的转移和抗菌药物敏感性的变化 1011。一般来说,福氏志贺菌和宋内志贺菌是主要的病原体,并且对抗菌药物敏感性的变化有很大的影响 1213。本研究确定了与加拿大艾伯塔省旅行者感染福氏志贺菌和宋内志贺菌相关的全球区域,并比较了这些分离株 2002 年至 2007 年的抗生素耐药模式。2002 年至 2007 年(含)期间从加拿大艾伯塔省福氏志贺菌和宋内志贺菌感染患者中采集的标本进行了研究。标本送检时收集的数据包括:标本采集日期、是否存在暴发关联(如果有)、旅行史和药敏试验(数据来源:ProvLab 信息系统;艾伯塔省卫生和健康传染病报告)。公共卫生官员将暴发定义为≥ 2 例具有流行病学相关性的病例。每个暴发都被分配了一个唯一的事件编号。在原始病例感染后 6 个月内收到的重复分离株被排除在外。每个暴发只包括一个有代表性的病例,除非分离株具有不同的抗生素敏感性模式。根据旅行史,将分离株的来源分为相应的地区和大陆。本研究中包含的地区代表了居住在加拿大的个人的主要旅行目的地。国内暴露被定义为“在北美境内旅行”。