The Alan Edwards Centre for Research on Pain, McGill University, 740, Dr, Penfield Ave, Montreal, Quebec, H3A 2B2, Canada.
Mol Pain. 2010 Nov 10;6:79. doi: 10.1186/1744-8069-6-79.
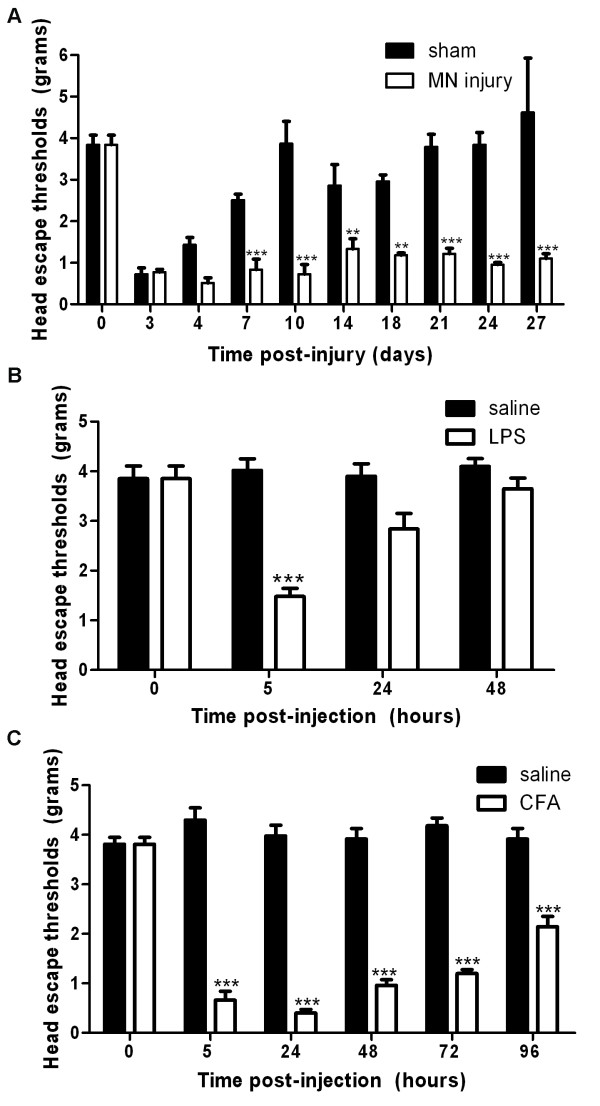
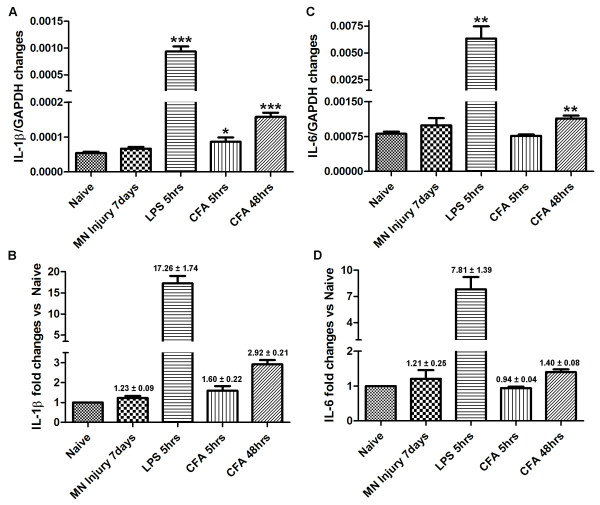
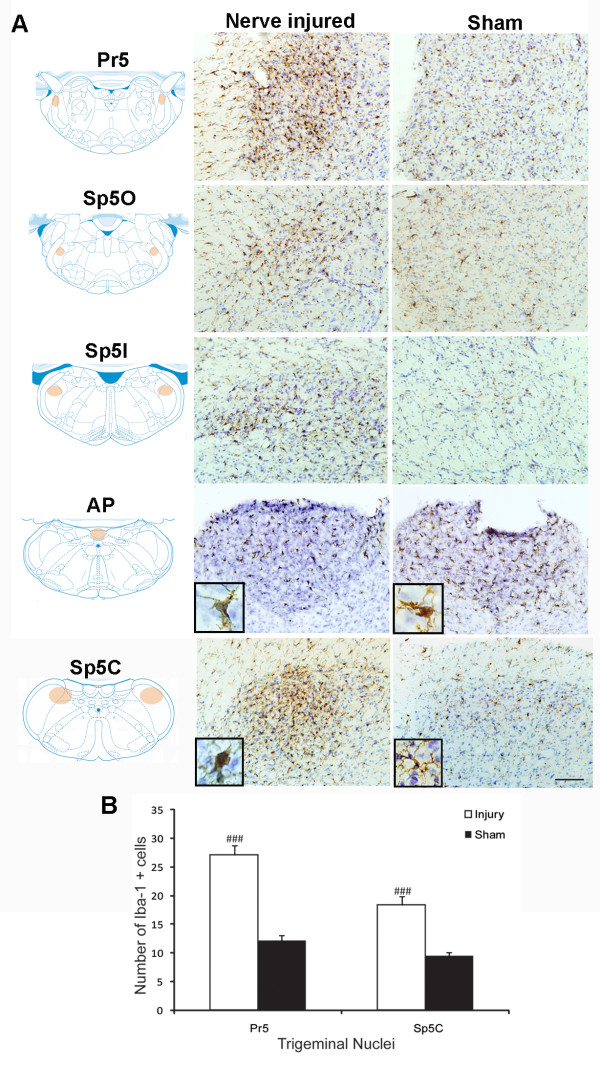
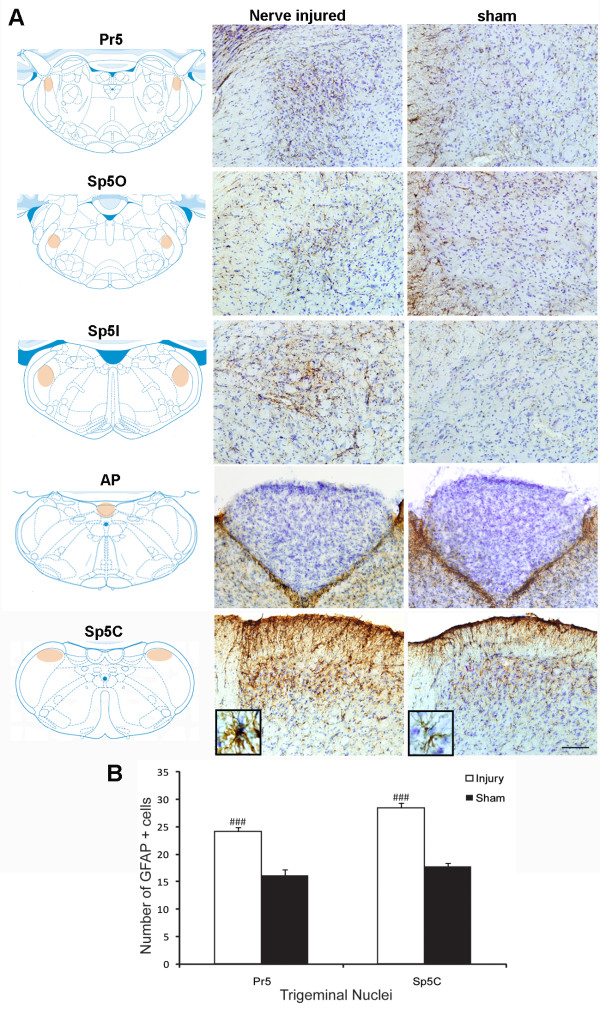
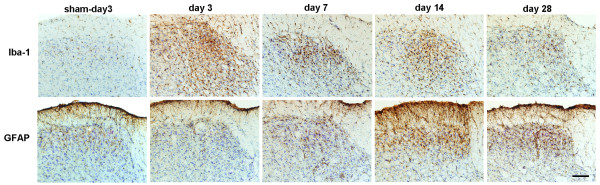
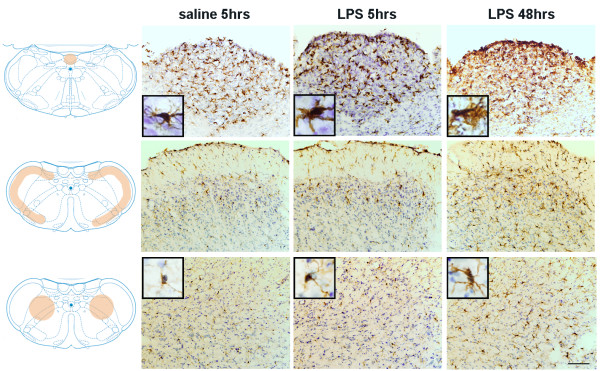
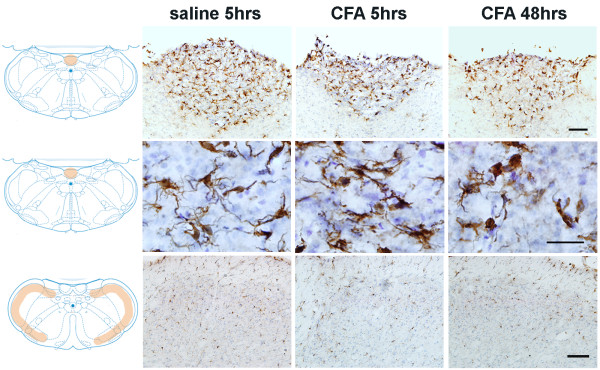
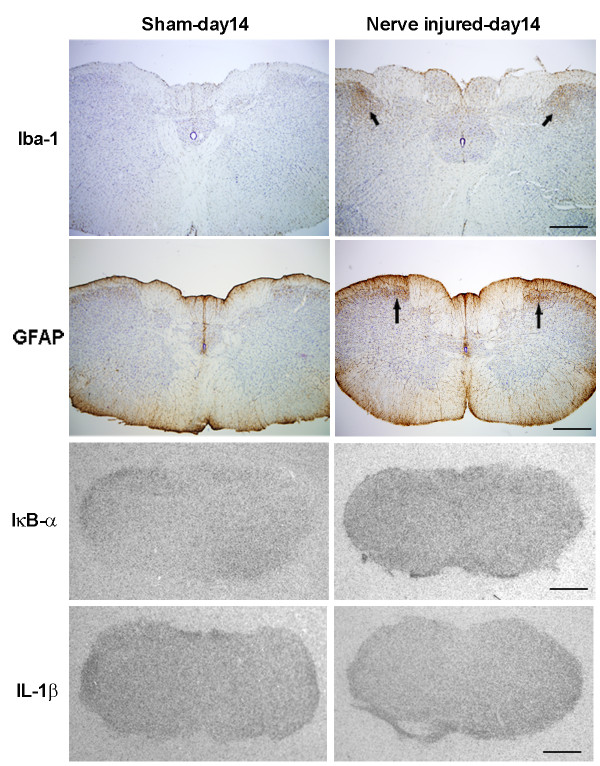
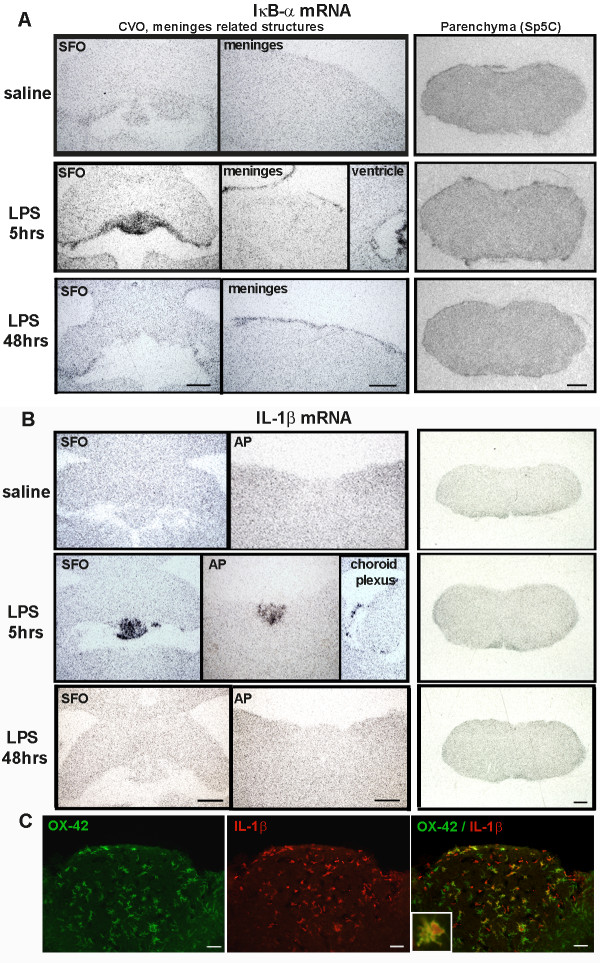
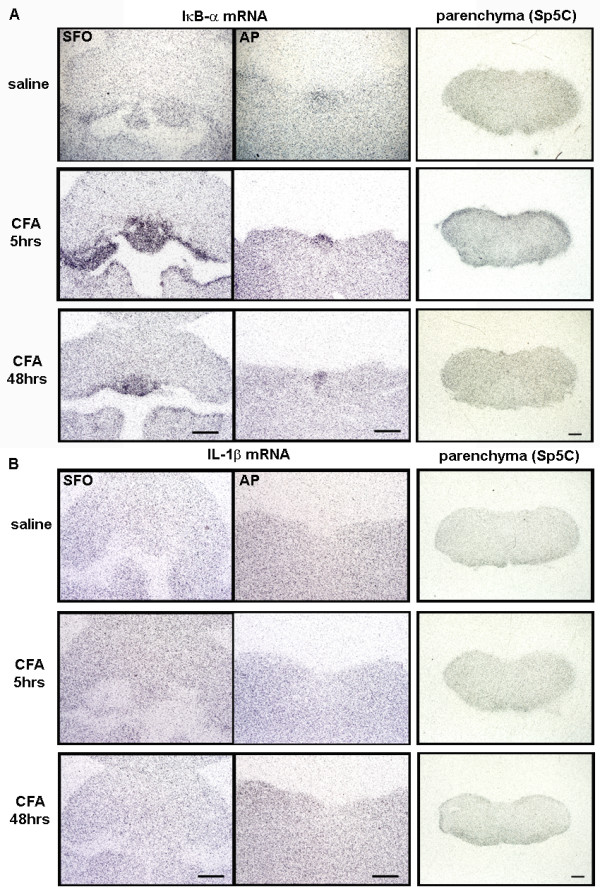
Oro-facial pain following injury and infection is frequently observed in dental clinics. While neuropathic pain evoked by injury associated with nerve lesion has an involvement of glia/immune cells, inflammatory hyperalgesia has an exaggerated sensitization mediated by local and circulating immune mediators. To better understand the contribution of central nervous system (CNS) glial cells in these different pathological conditions, in this study we sought to characterize functional phenotypes of glial cells in response to trigeminal nerve injury (loose ligation of the mental branch), infection (subcutaneous injection of lipopolysaccharide--LPS) and to sterile inflammation (subcutaneous injection of complete Freund's adjuvant--CFA) on the lower lip. Each of the three insults triggered a specific pattern of mechanical allodynia. In parallel with changes in sensory response, CNS glial cells reacted distinctively to the challenges. Following ligation of the mental nerve, both microglia and astrocytes in the trigeminal nuclear complex were highly activated, more prominent in the principal sensory nucleus (Pr5) and subnucleus caudalis (Sp5C) area. Microglial response was initiated early (days 3-14), followed by delayed astrocytes activation (days 7-28). Although the temporal profile of microglial and astrocyte reaction corresponded respectively to the initiation and chronic stage of neuropathic pain, these activated glial cells exhibited a low profile of cytokine expression. Local injection of LPS in the lower lip skin also triggered a microglial reaction in the brain, which started in the circumventricular organs (CVOs) at 5 hours post-injection and diffused progressively into the brain parenchyma at 48 hours. This LPS-induced microglial reaction was accompanied by a robust induction of IκB-α mRNA and pro-inflammatory cytokines within the CVOs. However, LPS induced microglial activation did not specifically occur along the pain signaling pathway. In contrast, CFA injection led to minor microglial morphological changes and an induction of IκB-α mRNA in the CVO regions; a significant increase in IL-1β and IL-6 mRNA started only at 48 hours post-injection, when the induced pain-related behavior started to resolve. Our detailed analysis of CNS glial response clearly revealed that both nerve injury and oro-facial infection/inflammation induced CNS glial activation, but in a completely different pattern, which suggests a remarkable plasticity of glial cells in response to dynamic changes in their microenvironment and different potential involvement of this non-neuronal cell population in pathological pain development.
口腔颌面部疼痛是口腔诊所中常见的问题。口腔颌面部疼痛通常是由创伤和感染引起的。口腔颌面部疼痛通常是由创伤和感染引起的,而创伤引起的神经病理性疼痛与神经损伤有关,涉及胶质细胞/免疫细胞,而炎症性痛觉过敏则由局部和循环免疫介质介导的过度敏感化引起。为了更好地理解中枢神经系统(CNS)胶质细胞在这些不同病理条件下的贡献,本研究试图描述三叉神经损伤(下颌支松散结扎)、感染(脂多糖皮下注射-LPS)和无菌性炎症(完全弗氏佐剂-CFA 皮下注射)下唇时,胶质细胞的功能表型。这三种刺激都触发了特定的机械性痛觉过敏模式。与感觉反应的变化平行,中枢神经系统胶质细胞对这些挑战有明显的反应。在结扎下颌神经后,三叉神经核复合体中的小胶质细胞和星形胶质细胞均被高度激活,在主感觉核(Pr5)和尾状核下区(Sp5C)区域更为明显。小胶质细胞的反应是早期开始的(第 3-14 天),随后是星形胶质细胞的延迟激活(第 7-28 天)。尽管小胶质细胞和星形胶质细胞反应的时间模式分别对应于神经病理性疼痛的起始和慢性阶段,但这些激活的胶质细胞表现出低水平的细胞因子表达。局部注射 LPS 在下唇皮肤也会在大脑中引发小胶质细胞反应,该反应始于脑室周围器官(CVOs),在注射后 5 小时开始扩散,并在 48 小时内逐渐扩散到脑实质。这种 LPS 诱导的小胶质细胞反应伴随着 CVOs 中 IκB-α mRNA 和促炎细胞因子的强烈诱导。然而,LPS 诱导的小胶质细胞激活并不是沿着疼痛信号通路特异性发生的。相比之下,CFA 注射仅导致 CVO 区域的小胶质细胞形态学变化和 IκB-α mRNA 的诱导;只有在注射后 48 小时,即诱导的疼痛相关行为开始缓解时,IL-1β 和 IL-6 mRNA 的显著增加才开始。我们对中枢神经系统胶质细胞反应的详细分析清楚地表明,神经损伤和口腔颌面部感染/炎症都会导致中枢神经系统胶质细胞激活,但模式完全不同,这表明胶质细胞对其微环境的动态变化具有显著的可塑性,并且这种非神经元细胞群体在病理性疼痛发展中的潜在参与程度也不同。