Department of Radiation Oncology, Duke University Medical Center, Durham, NC, USA.
Radiother Oncol. 2010 Dec;97(3):535-40. doi: 10.1016/j.radonc.2010.10.020. Epub 2010 Nov 11.
Chest wall recurrences of breast cancer are a therapeutic challenge and durable local control is difficult to achieve. Our objective was to determine the local progression free survival (LPFS) and toxicity of thermochemoradiotherapy (ThChRT) for chest wall recurrence.
Twenty-seven patients received ThChRT for chest wall failure from 2/1995 to 6/2007 and make up this retrospective series. All received concurrent superficial hyperthermia twice weekly (median 8 sessions), chemotherapy (capecitabine in 21, vinorelbine in 2, and paclitaxel in 4), and radiation (median 45 Gy). Patients were followed up every 1.5-3 months and responses were graded with RECIST criteria and toxicities with the NCI CTC v4.0.
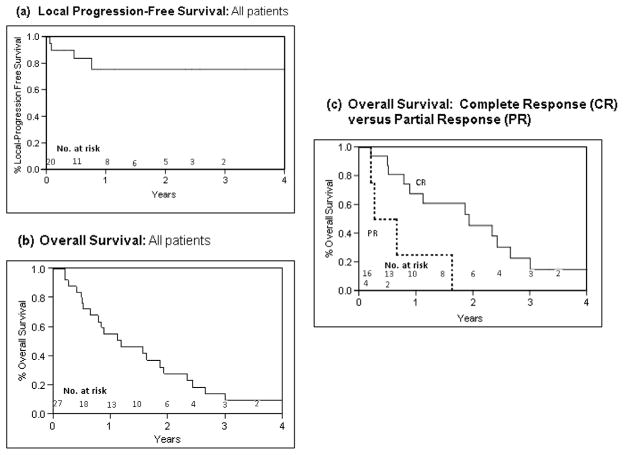
Twenty-three (85%) patients were previously irradiated (median 60.4 Gy) and 22 (81%) patients received prior chemotherapy. Median follow-up was 11 months. Complete response (CR) was achieved in 16/20 (80%) of patients with follow-up data, and 1 year LPFS was 76%. Overall survival was 23 months for patients with CR, and 5.4 months in patients achieving a partial response (PR) (p=0.01). Twenty-two patients experienced acute grade 1/2 treatment related toxicities, primarily moist desquamation. Two patients experienced 3rd degree burns; all resolved with conservative measures.
ThChRT offers durable palliation and prolonged LPFS with tolerable acute toxicity, especially if CR is achieved.
乳腺癌胸壁复发是一个治疗挑战,难以实现持久的局部控制。我们的目的是确定热化疗放疗(ThChRT)治疗胸壁复发的局部无进展生存期(LPFS)和毒性。
27 例患者于 1995 年 2 月至 2007 年 6 月因胸壁失败接受 ThChRT,构成了本回顾性系列研究。所有患者均接受每周两次的浅表高温治疗(中位数为 8 次)、化疗(卡培他滨 21 例、长春瑞滨 2 例、紫杉醇 4 例)和放疗(中位数 45 Gy)。患者每 1.5-3 个月随访一次,采用 RECIST 标准评估疗效,采用 NCI CTC v4.0 评估毒性。
23 例(85%)患者既往接受过放疗(中位数 60.4 Gy),22 例(81%)患者接受过化疗。中位随访时间为 11 个月。有随访数据的 20 例患者中,16 例(80%)达到完全缓解(CR),1 年 LPFS 为 76%。CR 患者的总生存期为 23 个月,部分缓解(PR)患者的总生存期为 5.4 个月(p=0.01)。22 例患者出现急性 1/2 级治疗相关毒性,主要为湿性脱皮。2 例患者发生 3 度烧伤;所有患者均通过保守治疗治愈。
ThChRT 提供了持久的缓解和延长的 LPFS,同时具有可耐受的急性毒性,尤其是在达到 CR 的情况下。