Intensive Care Unit and Postgraduate Program, Instituto Nacional de Câncer, 10° Andar; Praça Cruz Vermelha, 23; Rio de Janeiro-RJ; CEP: 20230-130, Brazil.
Crit Care. 2010;14(6):R210. doi: 10.1186/cc9333. Epub 2010 Nov 23.
Delirium is a frequent source of morbidity in intensive care units (ICUs). Most data on its epidemiology is from single-center studies. Our aim was to conduct a multicenter study to evaluate the epidemiology of delirium in the ICU.
A 1-day point-prevalence study was undertaken in 104 ICUs from 11 countries in South and North America and Spain.
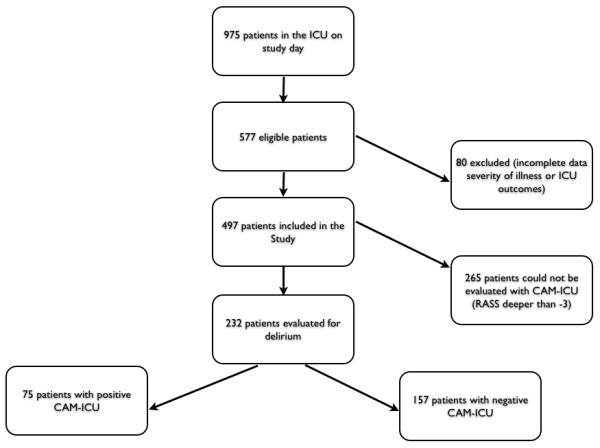
In total, 975 patients were screened, and 497 fulfilled inclusion criteria and were enrolled (median age, 62 years; 52.5% men; 16.7% and 19.9% for ICU and hospital mortality); 64% were admitted to the ICU because of medical causes, and sepsis was the main diagnosis (n = 76; 15.3%). In total, 265 patients were sedated with the Richmond agitation and sedation scale (RASS) deeper than -3, and only 232 (46.6%) patients could be evaluated with the confusion-assessment method for the ICU. The prevalence of delirium was 32.3%. Compared with patients without delirium, those with the diagnosis of delirium had a greater severity of illness at admission, demonstrated by higher sequential organ-failure assessment (SOFA (P = 0.004)) and simplified acute physiology score 3 (SAPS3) scores (P < 0.0001). Delirium was associated with increased ICU (20% versus 5.7%; P = 0.002) and hospital mortality (24 versus 8.3%; P = 0.0017), and longer ICU (P < 0.0001) and hospital length of stay (LOS) (22 (11 to 40) versus 7 (4 to 18) days; P < 0.0001). Previous use of midazolam (P = 0.009) was more frequent in patients with delirium. On multivariate analysis, delirium was independently associated with increased ICU mortality (OR = 3.14 (1.26 to 7.86); CI, 95%) and hospital mortality (OR = 2.5 (1.1 to 5.7); CI, 95%).
In this 1-day international study, delirium was frequent and associated with increased mortality and ICU LOS. The main modifiable risk factors associated with the diagnosis of delirium were the use of invasive devices and sedatives (midazolam).
谵妄是重症监护病房(ICU)发病率较高的一个因素。大多数关于其流行病学的数据都来自单中心研究。我们的目的是开展一项多中心研究,评估 ICU 谵妄的流行病学情况。
在 11 个南美、北美和西班牙国家的 104 个 ICU 进行了为期 1 天的患病率研究。
共筛选了 975 名患者,其中 497 名符合纳入标准并被纳入研究(中位年龄 62 岁;52.5%为男性;ICU 和医院死亡率分别为 16.7%和 19.9%);64%的患者因医疗原因入住 ICU,其中主要诊断为脓毒症(n=76;15.3%)。共有 265 名患者使用 Richmond 躁动和镇静量表(RASS)镇静程度超过-3,仅有 232 名(46.6%)患者可以使用 ICU 意识模糊评估法进行评估。谵妄的患病率为 32.3%。与没有谵妄的患者相比,诊断为谵妄的患者入院时的疾病严重程度更高,表现为序贯器官衰竭评估(SOFA(P=0.004))和简化急性生理学评分 3 (SAPS3)评分更高(P<0.0001)。谵妄与 ICU(20%比 5.7%;P=0.002)和医院死亡率(24 比 8.3%;P=0.0017)增加相关,且 ICU(P<0.0001)和医院住院时间(LOS)(22(11 至 40)比 7(4 至 18)天;P<0.0001)延长。谵妄患者中咪达唑仑的使用更为频繁(P=0.009)。多变量分析显示,谵妄与 ICU 死亡率增加独立相关(OR=3.14(1.26 至 7.86);95%CI)和医院死亡率增加独立相关(OR=2.5(1.1 至 5.7);95%CI)。
在这项为期 1 天的国际研究中,谵妄较为常见,且与死亡率增加和 ICU LOS 延长相关。与谵妄诊断相关的主要可改变危险因素是使用有创设备和镇静剂(咪达唑仑)。