Physiological Laboratory, Department of Biochemistry, University of Cambridge, Downing Site, Cambridge CB2 3EG, UK.
Am J Physiol Heart Circ Physiol. 2011 Feb;300(2):H605-16. doi: 10.1152/ajpheart.00824.2010. Epub 2010 Nov 19.
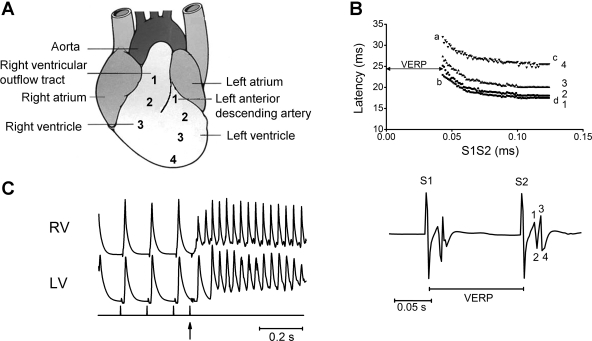
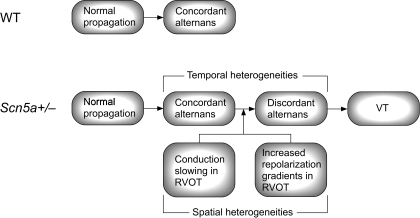
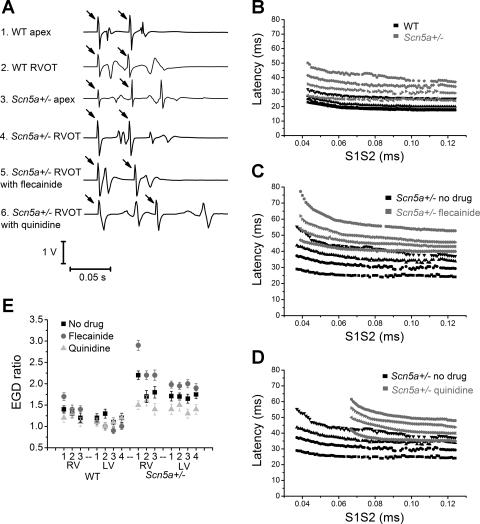
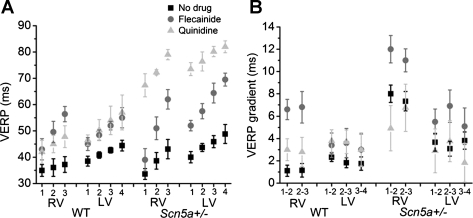
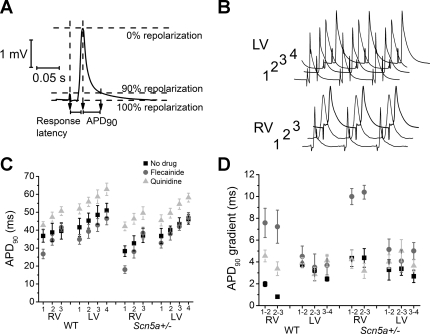
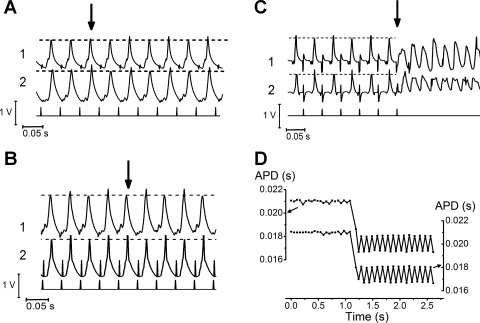
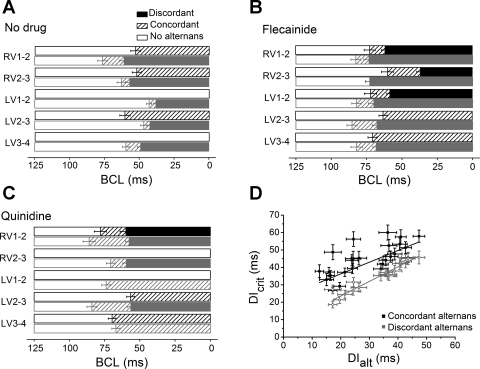
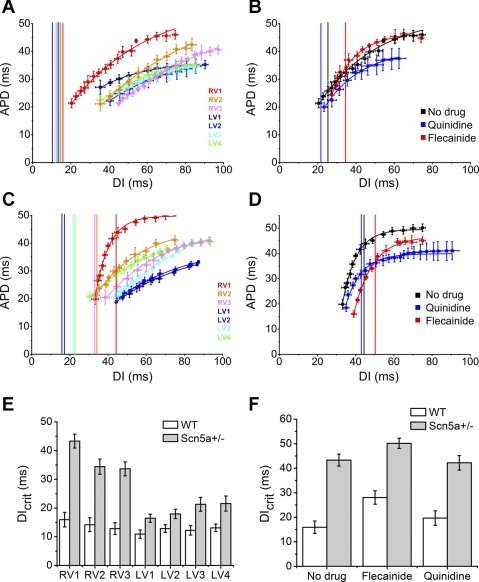
Ventricular tachycardia (VT) in Brugada Syndrome patients often originates in the right ventricular outflow tract (RVOT). We explore the physiological basis for this observation using murine whole heart preparations. Ventricular bipolar electrograms and monophasic action potentials were recorded from seven epicardial positions in Langendorff-perfused wild-type and Scn5a+/- hearts. VT first appeared in the RVOT, implicating it as an arrhythmogenic focus in Scn5a+/- hearts. RVOTs showed the greatest heterogeneity in refractory periods, response latencies, and action potential durations, and the most fractionated electrograms. However, incidences of concordant alternans in dynamic pacing protocol recordings were unaffected by the Scn5a+/- mutation or pharmacological intervention. Conversely, particularly at the RVOT, Scn5a+/- hearts showed earlier and more frequent transitions into discordant alternans. This was accentuated by flecainide, but reduced by quinidine, in parallel with their respective pro- and anti-arrhythmic effects. Discordant alternans preceded all episodes of VT. The RVOT of Scn5a+/- hearts also showed steeper restitution curves, with the diastolic interval at which the gradient equaled one strongly correlating with the diastolic interval at which discordant alternans commenced. We attribute the arrhythmic tendency within the RVOT to the greater spatial heterogeneities in baseline electrophysiological properties. These, in turn, give rise to a tendency to drive concordant alternans phenomena into an arrhythmogenic discordant alternans. Our findings may contribute to future work investigating possible pharmacological treatments for a disease in which the current mainstay of treatment is implantable cardioverter defibrillator implantation.
Brugada 综合征患者的室性心动过速 (VT) 通常起源于右心室流出道 (RVOT)。我们使用鼠全心制剂探索这一观察结果的生理基础。在 Langendorff 灌注的野生型和 Scn5a+/- 心脏的七个心外膜位置记录心室双极电图和单相动作电位。VT 首先出现在 RVOT 中,表明其为 Scn5a+/- 心脏的致心律失常焦点。RVOT 在不应期、反应潜伏期和动作电位持续时间方面表现出最大的异质性,并且具有最分散的电图。然而,动态起搏方案记录中一致性交替的发生率不受 Scn5a+/- 突变或药物干预的影响。相反,特别是在 RVOT,Scn5a+/- 心脏显示出更早和更频繁的不一致性交替。这在氟卡尼的作用下更为明显,但在奎尼丁的作用下减轻,与它们各自的抗心律失常和致心律失常作用平行。不一致性交替先于所有 VT 发作。Scn5a+/- 心脏的 RVOT 还显示出更陡的复极曲线,其中斜率等于 1 的舒张间隔与开始不一致性交替的舒张间隔强烈相关。我们将 RVOT 中的心律失常倾向归因于基线电生理特性的更大空间异质性。反过来,这导致倾向于将一致的交替现象驱动为致心律失常的不一致交替。我们的发现可能有助于未来研究可能的药物治疗这种疾病的工作,目前这种疾病的主要治疗方法是植入式心脏复律除颤器植入。