Kim Sang-Bum, Jeon Taek-Soo, Lee Woo-Suk, Roh Jae-Young, Kim Jae-Young, Park Won-Ki
Department of Orthopaedic Surgery, Konyang University College of Medicine, Daejeon, Korea.
Asian Spine J. 2010 Dec;4(2):102-8. doi: 10.4184/asj.2010.4.2.102. Epub 2010 Nov 24.
A retrospective study.
To compare the level of restoration of the vertebral height, improvement in the wedge and kyphotic angles, and the incidence of complications in osteoporotic compression fracture in patients treated with either kyphoplasty or lordoplasty.
Kyphoplasty involves recompression of the vertebral bodies. Recently, a more effective method known as lordoplasty was introduced.
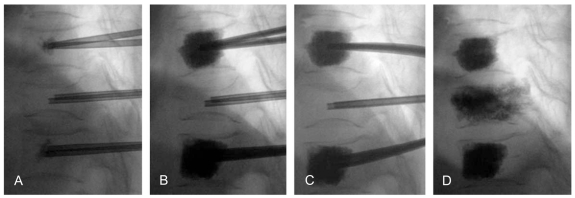
Between 2004 and 2009, patients with osteoporotic thoracolumbar vertebral compression fractures were treated by either kyphoplasty (n = 24) or lordoplasty (n = 12) using polymethylmethacrylate (PMMA) cement, and the results of the two interventions were compared. A visual analogue scale was used to measure the pain status. Preoperative and postoperative radiographs were analyzed to quantify the anterior vertebral height restoration and the wedge and kyphotic alignment correction.
All patients in both groups reported a significant decrease in pain. The anterior heights increased 24.2% and 17.5% after the lordoplasty and kyphoplasty procedures, respectively (p < 0.05). Three months after the procedures, there was a larger decrease in the loss of anterior vertebral height in the kyphoplasty group (12.8%) than in the lordoplasty group (6.3%, p < 0.05). The wedge angles decreased after both procedures. The wedge angle in the lordoplasty group maintained its value after 3 months (p < 0.05). The kyphotic angular correction was 11.4 and 7.0° in the lordoplasty and kyphoplasty groups, respectively (p < 0.05). Both kyphotic deformities worsened to a similar degree of 5° after 3 months.
Lordoplasty is more useful than kyphoplasty in terms of the improved anatomic restoration and postoperative maintenance.
一项回顾性研究。
比较经椎体后凸成形术或椎体前凸成形术治疗的骨质疏松性压缩骨折患者的椎体高度恢复水平、楔角和后凸角改善情况以及并发症发生率。
椎体后凸成形术包括对椎体进行再压缩。最近,一种更有效的方法即椎体前凸成形术被引入。
2004年至2009年期间,采用聚甲基丙烯酸甲酯(PMMA)骨水泥对骨质疏松性胸腰椎椎体压缩骨折患者分别进行椎体后凸成形术(n = 24)或椎体前凸成形术(n = 12)治疗,并比较两种干预措施的结果。采用视觉模拟量表测量疼痛状况。分析术前和术后X线片以量化椎体前缘高度恢复情况以及楔角和后凸对线矫正情况。
两组所有患者均报告疼痛显著减轻。椎体前凸成形术和椎体后凸成形术后椎体前缘高度分别增加了24.2%和17.5%(p < 0.05)。术后3个月,椎体后凸成形术组椎体前缘高度丢失的减少幅度(12.8%)大于椎体前凸成形术组(6.3%,p < 0.05)。两种手术后楔角均减小。椎体前凸成形术组术后3个月楔角保持不变(p < 0.05)。椎体前凸成形术组和椎体后凸成形术组的后凸角矫正分别为11.4°和7.0°(p < 0.05)。3个月后,两种后凸畸形均恶化至相似的5°程度。
在改善解剖复位和术后维持方面,椎体前凸成形术比椎体后凸成形术更有用。