Department of Internal Medicine, Catholic University, Rome, Italy.
Diabetes Care. 2011 Mar;34(3):561-7. doi: 10.2337/dc10-1761. Epub 2011 Jan 31.
The surgical option could represent a valid alternative to medical therapy in some diabetic patients. However, no data are available on long-term effects of metabolic surgery on diabetic complications. We aimed to determine whether patients with newly diagnosed type 2 diabetes who underwent bilio-pancreatic diversion (BPD) had less micro- and macrovascular complications than those who received conventional therapy.
This was an unblinded, case-controlled trial with 10-years' follow-up, conducted from July 1998 through October 2009 at the Day Hospital of Metabolic Diseases, Catholic University, Rome, Italy. A consecutive sample of 110 obese patients (BMI >35 kg/m(2)) with newly diagnosed type 2 diabetes was enrolled. The study was completed by 50 subjects. The main outcome measure was long-term effects (10 years) of BPD versus those associated with conventional therapy on microvascular outcome, micro- and macroalbuminuria, and glomerular filtration rate (GFR). Secondary measures included macrovascular outcomes, type 2 diabetes remission, glycated hemoglobin, and hyperlipidemia.
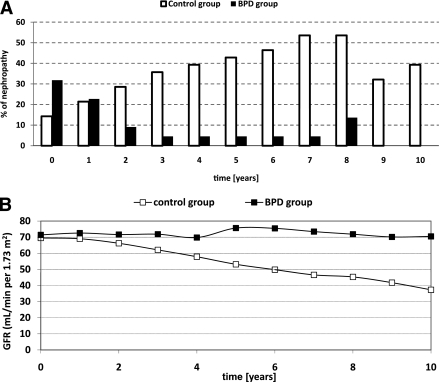
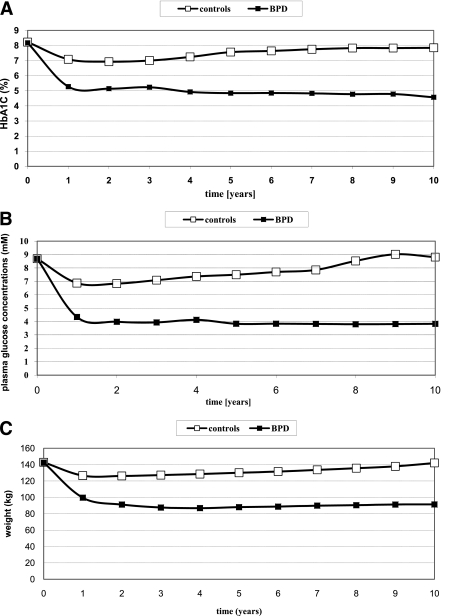
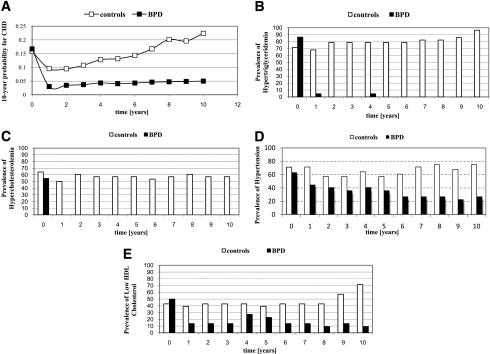
Ten-year GFR variation was -45.7 ± 18.8% in the medical arm and 13.6 ± 24.5% in the surgical arm (P < 0.001). Ten-year hypercreatininemia prevalence was 39.3% in control subjects and 9% in BPD subjects (P = 0.001). After 10 years, all BPD subjects recovered from microalbuminuria, whereas microalbuminuria appeared or progressed to macroalbuminuria in control subjects. Three myocardial infarctions, determined by electrocardiogram, and one stroke occurred in control subjects. After the 10-year follow-up, coronary heart disease (CHD) probability was 0.22 ± 0.10 and 0.05 ± 0.04 in the medical and surgical groups, respectively (P < 0.001). Remission from type 2 diabetes was observed in all patients within 1 year of surgery. Surgical and medical subjects had lost 34.60 ± 10.25 and 0.38 ± 6.10% of initial weight at the 10-year follow-up (P < 0.001).
Renal and cardiovascular complications were dramatically reduced in the surgical arm, indicating long-term benefits of BPD on diabetic complications, at least in the case of morbid obesity with decompensated type 2 diabetes.
对于某些糖尿病患者,手术选择可能是医学治疗的有效替代方案。然而,关于代谢手术对糖尿病并发症的长期影响的数据尚不可用。我们旨在确定新诊断为 2 型糖尿病的患者接受胆胰分流术(BPD)是否比接受常规治疗的患者发生微血管和大血管并发症的风险更低。
这是一项从 1998 年 7 月至 2009 年 10 月在意大利罗马天主教大学代谢疾病日间医院进行的非盲、病例对照试验,随访 10 年。一项连续样本包括 110 名肥胖(BMI>35kg/m²)新诊断为 2 型糖尿病的患者。该研究完成了 50 例患者。主要观察指标是 BPD 与常规治疗对微血管结果、微量白蛋白尿和大蛋白尿以及肾小球滤过率(GFR)的长期影响(10 年)。次要观察指标包括大血管结果、2 型糖尿病缓解、糖化血红蛋白和血脂异常。
10 年时,药物组的 GFR 变化为-45.7±18.8%,手术组为 13.6±24.5%(P<0.001)。10 年时,对照组的高肌氨酸血症患病率为 39.3%,BPD 组为 9%(P=0.001)。10 年后,所有 BPD 患者的微量白蛋白尿均恢复正常,而对照组的微量白蛋白尿则出现或进展为大量白蛋白尿。对照组发生 3 次心电图确定的心肌梗死和 1 次中风。经过 10 年的随访,药物组和手术组的冠心病(CHD)概率分别为 0.22±0.10 和 0.05±0.04(P<0.001)。所有患者在手术后 1 年内均缓解了 2 型糖尿病。手术组和药物组患者在 10 年随访时分别减轻了初始体重的 34.60±10.25%和 0.38±6.10%(P<0.001)。
手术组的肾脏和心血管并发症明显减少,表明 BPD 对糖尿病并发症具有长期益处,至少在伴有代偿失调的 2 型糖尿病和病态肥胖的情况下是如此。