Ottawa Hospital Research Institute, Clinical Epidemiology Program, The Ottawa Hospital - Civic Campus, 1053 Carling Avenue, Room F-658, Ottawa, ON, K1Y 4E9, Canada.
BMC Emerg Med. 2011 Feb 1;11:1. doi: 10.1186/1471-227X-11-1.
Canadian Emergency Medical Services annually transport 1.3 million patients with potential neck injuries to local emergency departments. Less than 1% of those patients have a c-spine fracture and even less (0.5%) have a spinal cord injury. Most injuries occur before the arrival of paramedics, not during transport to the hospital, yet most patients are transported in ambulances immobilized. They stay fully immobilized until a bed is available, or until physician assessment and/or X-rays are complete. The prolonged immobilization is often unnecessary and adds to the burden of already overtaxed emergency medical services systems and crowded emergency departments.
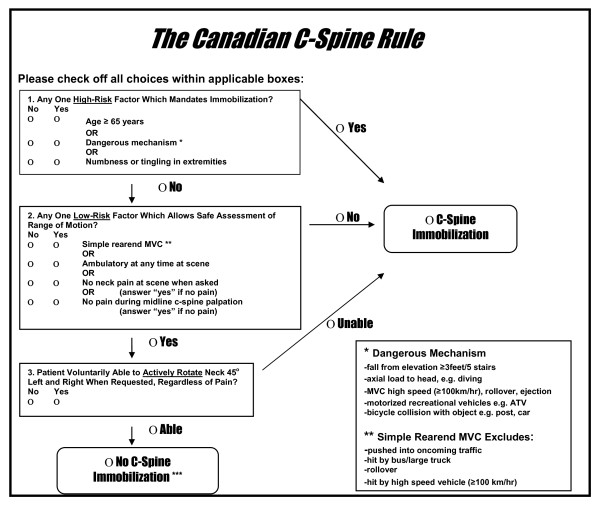
METHODS/DESIGN: The goal of this study is to evaluate the safety and potential impact of an active strategy that allows paramedics to assess very low-risk trauma patients using a validated clinical decision rule, the Canadian C-Spine Rule, in order to determine the need for immobilization during transport to the emergency department.This cohort study will be conducted in Ottawa, Canada with one emergency medical service. Paramedics with this service participated in an earlier validation study of the Canadian C-Spine Rule. Three thousand consecutive, alert, stable adult trauma patients with a potential c-spine injury will be enrolled in the study and evaluated using the Canadian C-Spine Rule to determine the need for immobilization. The outcomes that will be assessed include measures of safety (numbers of missed fractures and serious adverse outcomes), measures of clinical impact (proportion of patients transported without immobilization, key time intervals) and performance of the Rule.
Approximately 40% of all very low-risk trauma patients could be transported safely, without c-spine immobilization, if paramedics were empowered to make clinical decisions using the Canadian C-Spine Rule. This safety study is an essential step before allowing all paramedics across Canada to selectively immobilize trauma victims before transport. Once safety and potential impact are established, we intend to implement a multi-centre study to study actual impact.
加拿大急救医疗服务每年向当地急诊部门转运 130 万例疑似颈部损伤的患者。这些患者中只有不到 1%有颈椎骨折,更少有(0.5%)有脊髓损伤。大多数损伤发生在护理人员到达之前,而不是在送往医院的过程中,但大多数患者在救护车中都被固定。他们保持完全固定,直到有床位可用,或者医生评估和/或 X 射线检查完成。长时间的固定通常是不必要的,这增加了已经不堪重负的紧急医疗服务系统和拥挤的急诊部门的负担。
方法/设计:本研究的目的是评估一种主动策略的安全性和潜在影响,该策略允许护理人员使用经过验证的临床决策规则(加拿大颈椎规则)对低危创伤患者进行评估,以确定在送往急诊部的过程中是否需要固定。这项队列研究将在加拿大渥太华进行,由一家紧急医疗服务机构参与。该服务机构的护理人员参与了之前对加拿大颈椎规则的验证研究。研究将纳入 3000 例连续的、警觉的、稳定的成年创伤患者,他们有潜在的颈椎损伤,将使用加拿大颈椎规则进行评估,以确定是否需要固定。评估的结果将包括安全性指标(漏诊骨折和严重不良结局的数量)、临床影响指标(无固定运送的患者比例、关键时间间隔)和规则的表现。
如果护理人员能够使用加拿大颈椎规则做出临床决策,大约 40%的所有低危创伤患者可以安全地运送,无需颈椎固定。这项安全性研究是在允许加拿大各地的所有护理人员在转运前选择性固定创伤受害者之前的必要步骤。一旦安全性和潜在影响得到确定,我们打算进行一项多中心研究来研究实际影响。