Department of Endocrinology and Diabetes, School of Medicine, Saitama Medical University, 38 Morohongo, Moroyama-cho, Iruma-gun, Saitama 350-0495, Japan.
Diabetologia. 2011 May;54(5):1025-31. doi: 10.1007/s00125-010-2025-0. Epub 2011 Feb 1.
AIMS/HYPOTHESIS: The aim of the study was to determine the transition rate and factors associated with the progression of normo- and low microalbuminuria to diabetic nephropathy (overt proteinuria).
For 8 years we prospectively observed 1,558 Japanese patients with type 2 diabetes mellitus whose basal urinary albumin:creatinine ratio (UACR) had been measured as <17.0 mg/mmol at entry. The incidence of nephropathy (UACR >33.9 mg/mmol) was determined by measuring UACR twice a year.
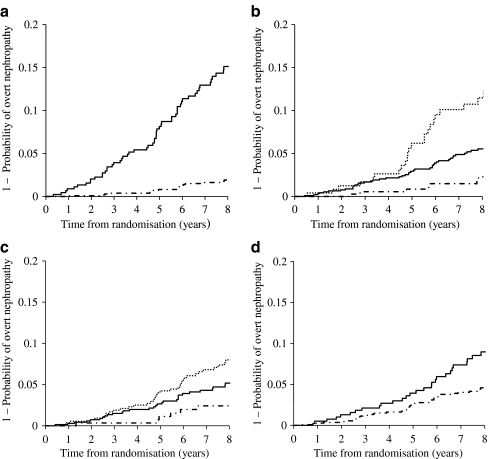
Progression to nephropathy occurred in 74 patients. The annual transition rate was 0.67%, and was substantially higher for the low-microalbuminuric group than for the normoalbuminuric group (1.85% and 0.23%, respectively; hazard ratio for the low-microalbuminuric group 8.45, p < 0.01). The hazard ratio for an HbA(1c) of 7-9% or ≥9% was 2.72 (p < 0.01) or 5.81 (p < 0.01) relative to HbA(1c) <7.0%, respectively. In comparison with individuals with a systolic blood pressure (SBP) of <120 mmHg, the hazard ratios for patients with an SBP of 120-140 mmHg or ≥140 mmHg were 2.31 (p = 0.06) and 3.54 (p < 0.01), respectively. Smoking also affected progression to proteinuria (hazard ratio 1.99, p < 0.01). In contrast, 30.3% of the low-microalbuminuric group returned to normoalbuminuria (i.e. were in remission).
CONCLUSIONS/INTERPRETATION: These results suggest that if patients with type 2 diabetes mellitus are receiving treatment from diabetologists for hyperglycaemia and hypertension when they are in the early stages of nephropathy (i.e. normo- or low microalbuminuria), their rate of transition to proteinuria is considerably lowered, and that differentiating patients with low microalbuminuria from those with high microalbuminuria might be clinically useful.
UMIN Clinical Trials Registry C000000222.
目的/假设:本研究旨在确定正常和微量白蛋白尿向糖尿病肾病(显性蛋白尿)进展的转化率以及相关因素。
我们前瞻性观察了 1558 名日本 2 型糖尿病患者,这些患者在入组时的基础尿白蛋白/肌酐比(UACR)<17.0mg/mmol。通过每年两次测量 UACR 来确定肾病(UACR>33.9mg/mmol)的发生率。
74 例患者进展为肾病。每年的转化率为 0.67%,微量白蛋白尿组的转化率明显高于正常白蛋白尿组(分别为 1.85%和 0.23%;微量白蛋白尿组的危险比为 8.45,p<0.01)。HbA1c 为 7-9%或≥9%的危险比分别为 2.72(p<0.01)或 5.81(p<0.01),与 HbA1c<7.0%相比。与收缩压(SBP)<120mmHg 的患者相比,SBP 为 120-140mmHg 或≥140mmHg 的患者的危险比分别为 2.31(p=0.06)和 3.54(p<0.01)。吸烟也会影响蛋白尿的进展(危险比 1.99,p<0.01)。相比之下,低微量白蛋白尿组有 30.3%的患者恢复正常白蛋白尿(即缓解)。
结论/解释:这些结果表明,如果 2 型糖尿病患者在肾病早期(即正常或微量白蛋白尿期)接受糖尿病专家治疗高血糖和高血压,其向蛋白尿转变的速度会显著降低,将低微量白蛋白尿患者与高微量白蛋白尿患者区分开来可能具有临床意义。
UMIN 临床试验注册 C000000222。