Department of Intensive Care, Radboud University Nijmegen Medical Centre PO Box 9101, 6500 HB Nijmegen, The Netherlands.
Crit Care. 2011;15(1):R48. doi: 10.1186/cc10012. Epub 2011 Feb 3.
Hypothermia may improve outcome in patients after traumatic brain injury, especially when hypothermia is maintained for more than 48 hours. In the acute phase, patients with severe brain injury are more vulnerable to infections. Prolonged hypothermic treatment may further enhance the risk of infection. Selective decontamination of the digestive tract (SDD) reduces the risk of respiratory tract infections. The aim of this study was to investigate the incidence of infections in patients treated with hypothermia and normothermia while receiving SDD.
In this retrospective case control study 35 patients treated with prolonged hypothermia (cases) were identified and 169 patients with severe brain injury were included (controls). Propensity score matching was performed to correct for differences in baseline characteristics and clinical parameters. Primary outcome was the incidence of infection. The secondary endpoints were the micro-organisms found in the surveillance cultures and infection. In addition, a number of clinical characteristics were assessed.
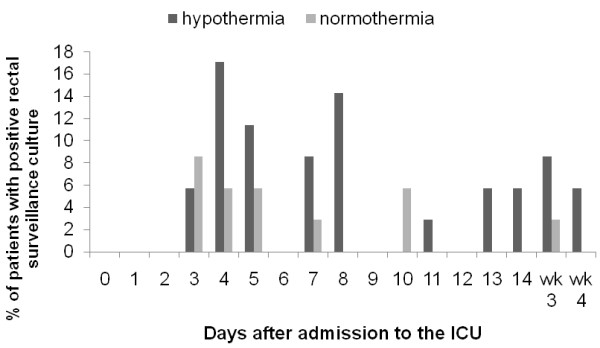
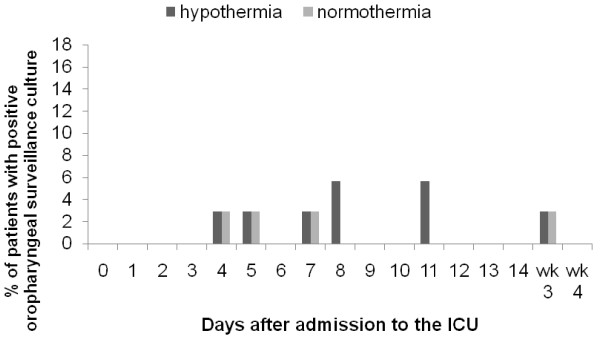
The demographic and clinical data indicated that the cases and controls were well matched. The overall risk of infection during ICU stay was 20% in the hypothermia groups versus 34.4% in the normothermia group (P = 0.388). Pneumonia was diagnosed in 11.4% of patients in both groups (P = 1.000). The incidence of meningitis, wound infection, bacteremia, and urinary tract infection was low and comparable between the groups. SDD surveillance cultures indicated a higher colonization with gram-negative bacteria in the rectal samples of the hypothermia patients.
Hypothermia does not increase the risk of infection in patients treated with SDD.
体温过低可能会改善创伤性脑损伤患者的预后,尤其是当体温过低持续超过 48 小时时。在急性期,严重脑损伤的患者更容易受到感染。长时间的低温治疗可能会进一步增加感染的风险。选择性消化道去污染(SDD)可降低呼吸道感染的风险。本研究旨在调查接受 SDD 治疗的低温和正常体温患者的感染发生率。
本回顾性病例对照研究中,确定了 35 例接受长时间低温治疗的患者(病例),并纳入了 169 例严重脑损伤患者(对照组)。采用倾向评分匹配法校正基线特征和临床参数的差异。主要结局是感染的发生率。次要终点是监测培养中发现的微生物和感染。此外,还评估了一些临床特征。
人口统计学和临床数据表明,病例组和对照组的情况匹配良好。在 ICU 住院期间,低温组的总感染风险为 20%,而正常体温组为 34.4%(P=0.388)。两组均有 11.4%的患者诊断为肺炎(P=1.000)。脑膜炎、伤口感染、菌血症和尿路感染的发生率较低,两组之间无差异。SDD 监测培养表明,低温组患者直肠样本中革兰氏阴性菌定植较高。
接受 SDD 治疗的患者中,低温不会增加感染的风险。