Division of Neurosurgery, Department of Surgery, Duke University Medical Center, Durham, North Carolina, United States of America.
PLoS One. 2011 Jan 26;6(1):e16031. doi: 10.1371/journal.pone.0016031.
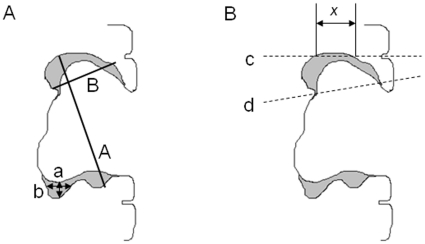
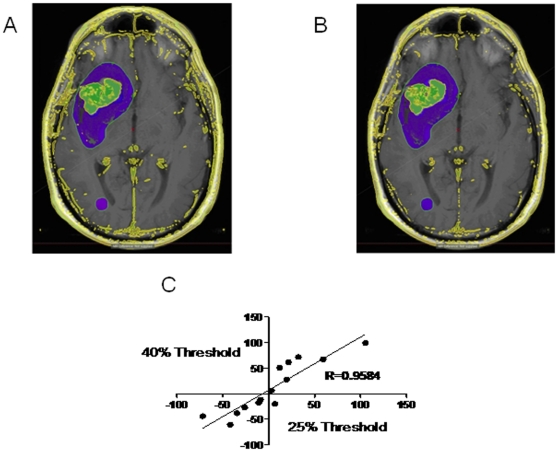
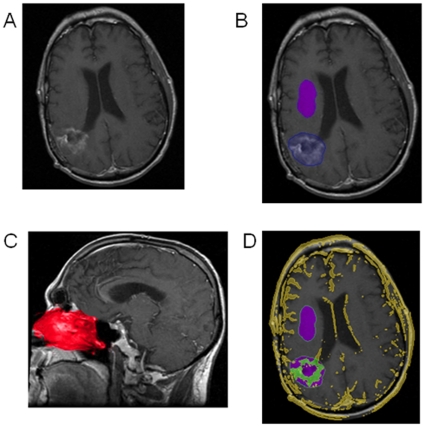
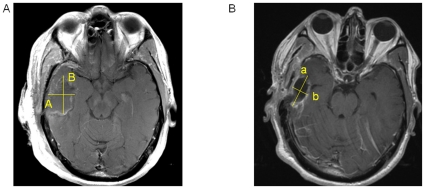
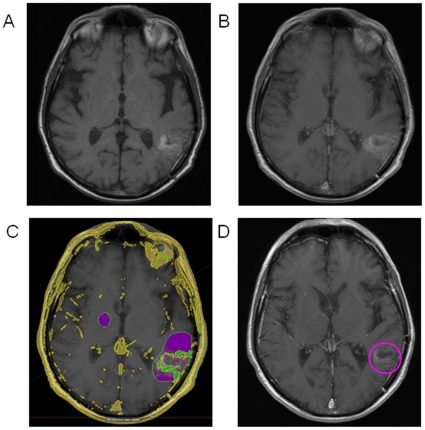
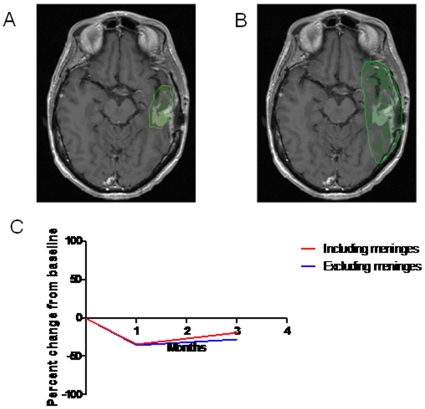
Current radiographic response criteria for brain tumors have difficulty describing changes surrounding postoperative resection cavities. Volumetric techniques may offer improved assessment, however usually are time-consuming, subjective and require expert opinion and specialized magnetic resonance imaging (MRI) sequences. We describe the application of a novel volumetric software algorithm that is nearly fully automated and uses standard T1 pre- and post-contrast MRI sequences. T1-weighted pre- and post-contrast images are automatically fused and normalized. The tumor region of interest is grossly outlined by the user. An atlas of the nasal mucosa is automatically detected and used to normalize levels of enhancement. The volume of enhancing tumor is then automatically calculated. We tested the ability of our method to calculate enhancing tumor volume with resection cavity collapse and when the enhancing tumor is obscured by subacute blood in a resection cavity. To determine variability in results, we compared narrowly-defined tumor regions with tumor regions that include adjacent meningeal enhancement and also compared different contrast enhancement threshold levels used for the automatic calculation of enhancing tumor volume. Our method quantified enhancing tumor volume despite resection cavity collapse. It detected tumor volume increase in the midst of blood products that incorrectly caused decreased measurements by other techniques. Similar trends in volume changes across scans were seen with inclusion or exclusion of meningeal enhancement and despite different automated thresholds for tissue enhancement. Our approach appears to overcome many of the challenges with response assessment of enhancing brain tumors and warrants further examination and validation.
目前,用于脑肿瘤的放射学反应标准在描述术后切除腔周围的变化方面存在困难。体积技术可能提供更好的评估,但通常耗时、主观,需要专家意见和专门的磁共振成像(MRI)序列。我们描述了一种新型的自动、几乎完全自动化的体积软件算法的应用,该算法使用标准的 T1 对比前后 MRI 序列。T1 加权前后图像自动融合和归一化。用户粗略勾勒肿瘤感兴趣区。自动检测鼻黏膜图谱并用于增强水平的归一化。然后自动计算增强肿瘤的体积。我们测试了我们的方法在切除腔塌陷和增强肿瘤被切除腔内亚急性血液遮挡时计算增强肿瘤体积的能力。为了确定结果的可变性,我们比较了狭窄定义的肿瘤区域与包括相邻脑膜增强的肿瘤区域,还比较了自动计算增强肿瘤体积时使用的不同对比增强阈值水平。尽管切除腔塌陷,我们的方法仍能定量增强肿瘤的体积。它检测到在血液产物中肿瘤体积的增加,而其他技术会错误地导致测量值降低。包括或排除脑膜增强以及不同的组织增强自动阈值对体积变化的相似趋势在不同扫描中均可见。我们的方法似乎克服了评估增强脑肿瘤反应的许多挑战,值得进一步研究和验证。