Coveney A P, O'Brien G C, Fulton G J
Department of Vascular Surgery, Cork University Hospital, National University of Ireland, Cork, Ireland.
Vasc Health Risk Manag. 2011 Jan 7;7:15-21. doi: 10.2147/VHRM.S15484.
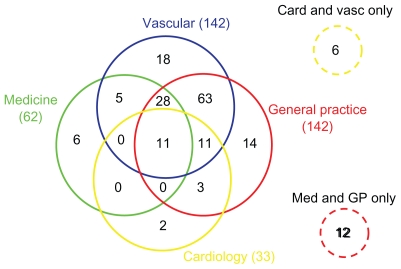
To examine the current medical management of arteriopathic patients attending a vascular surgical service at a university teaching hospital over a 6-month period. The prescribing of antiplatelets, statins, angiotensin-converting enzyme (ACE) inhibitors, or angiotensin receptor blockers and beta-blockers was specifically examined. Vascular patients are often under the care of multiple specialties, and therefore the influence of different medical specialties on the patients' medical management was also examined.
Between January and June 2009, data were recorded on sequential patients with arterial disease attending the vascular surgical service. Patients' demographics, type of arterial disease, medical consultations within the previous 12 months, and current medications were recorded.
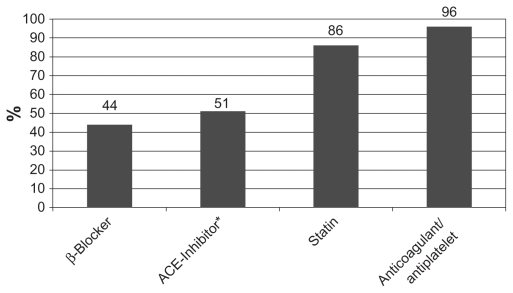
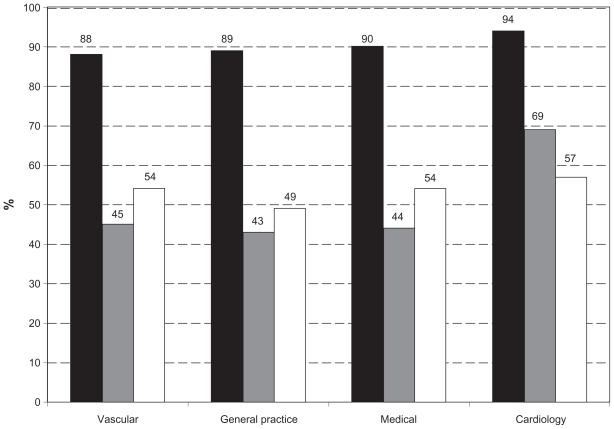
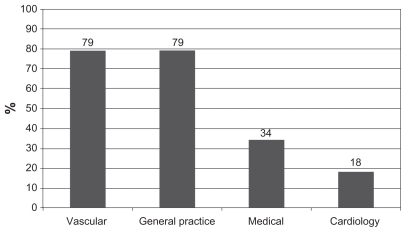
The study included 180 patients with a mean age of 69 years (39-88 years). All but 4% were taking an antiplatelet or anticoagulant, predominantly aspirin. There were 86% taking a statin, 44% taking a beta-blocker, and 51% taking an ACE inhibitor. Suboptimal prescription of ACE inhibitors and beta-blockers was evident regardless of the type of medical consultations in the previous year. No specialty group differed significantly from vascular surgeons in their prescribing pattern.
While almost all arteriopaths receive some form of antiplatelet and statin in line with clinical evidence, ACE inhibitors and beta-blockers appear to be under-prescribed in this arteriopathic population. We conclude that opportunity exists for vascular surgeons to embrace recent guidelines and lead the way in both surgical and medical optimization of arteriopathic patients through improving links with primary care physicians or taking greater responsibility themselves for the medical as well as the surgical care of their arteriopathic patients.
调查一所大学教学医院血管外科门诊6个月内动脉病变患者的当前药物治疗情况。具体考察抗血小板药物、他汀类药物、血管紧张素转换酶(ACE)抑制剂、血管紧张素受体阻滞剂及β受体阻滞剂的处方情况。血管疾病患者常由多个专科共同诊治,因此还考察了不同医学专科对患者药物治疗的影响。
2009年1月至6月,记录血管外科门诊连续就诊的动脉疾病患者的数据。记录患者的人口统计学信息、动脉疾病类型、过去12个月内的内科会诊情况及当前用药情况。
该研究纳入180例患者,平均年龄69岁(39 - 88岁)。除4%的患者外,其余均服用抗血小板药物或抗凝剂,主要为阿司匹林。86%的患者服用他汀类药物,44%的患者服用β受体阻滞剂,51%的患者服用ACE抑制剂。无论上一年的内科会诊类型如何,ACE抑制剂和β受体阻滞剂的处方都存在不合理之处。各专科组在处方模式上与血管外科医生无显著差异。
虽然几乎所有动脉病变患者都根据临床证据接受了某种形式的抗血小板药物和他汀类药物治疗,但在这一动脉病变人群中,ACE抑制剂和β受体阻滞剂的处方量似乎不足。我们得出结论,血管外科医生有机会采用最新指南,通过改善与基层医疗医生的联系或对动脉病变患者的内科及外科治疗承担更大责任,在动脉病变患者的外科和内科优化治疗方面发挥引领作用。