Department of Imaging, University Medical Center Utrecht, E01.132, P.O. Box 85500, 3508GA Utrecht, The Netherlands.
J Nucl Cardiol. 2011 Apr;18(2):238-46. doi: 10.1007/s12350-011-9339-2. Epub 2011 Feb 23.
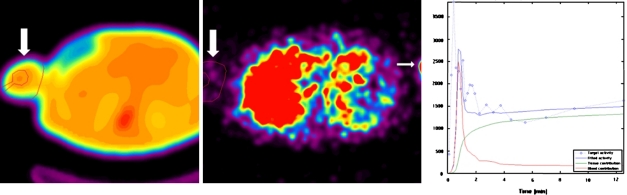
[13N]ammonia PET allows quantification of myocardial perfusion. The similarity between peripheral flow and myocardial perfusion is unclear. We compared perfusion flow in the myocardium with the upper limb during rest and adenosine stress [13N]ammonia PET to establish whether peripheral perfusion reserve (PPR) correlates with MPR.
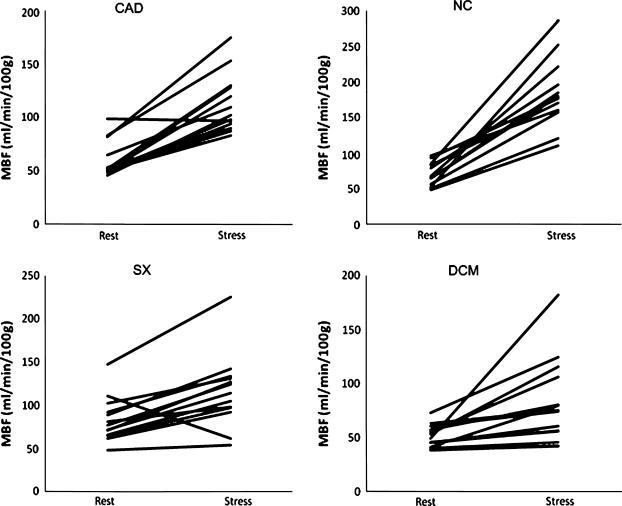
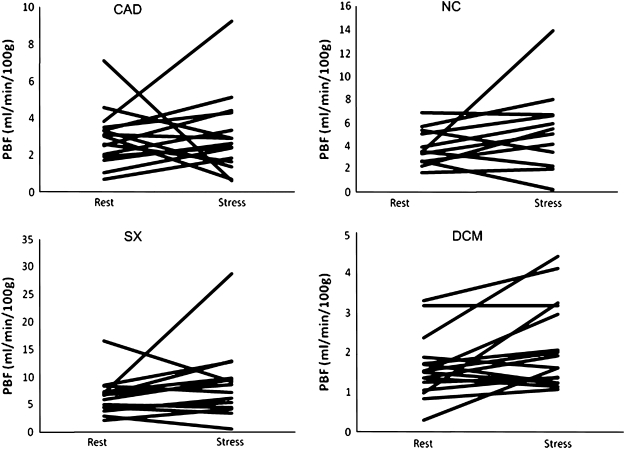
[13N]ammonia myocardial perfusion PET-scans of 58 patients were evaluated (27 men, 31 women, age 64 ± 13 years) and were divided in four subgroups: patients with coronary artery disease (CAD, n = 15), cardiac syndrome X (SX, n = 14), idiopathic dilating cardiomyopathy (DCM, n = 16), and normal controls (NC, n = 13). Peripheral limb perfusion was measured in the muscular tissue of the proximal upper limb and quantified through a 2-tissue-compartment model and the PPR was calculated (stress/rest ratio). MPR was also calculated by a 2-tissue-compartment model. The PPR results were compared with the MPR findings.
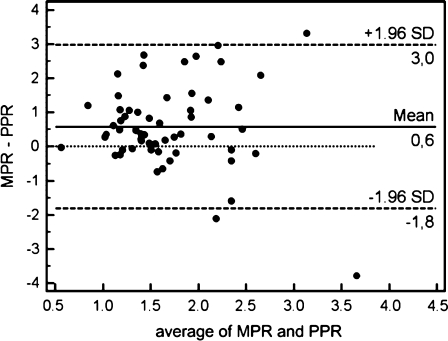
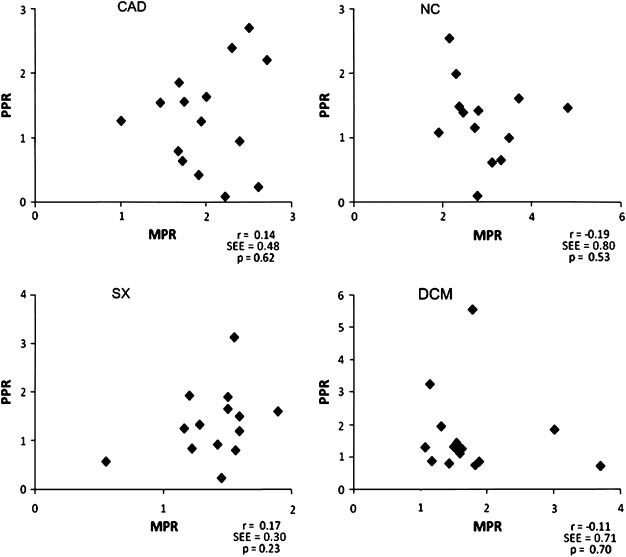
Mean myocardial perfusion increased significantly in all groups as evidenced by the MPR (CAD 1.99 ± 0.47; SX 1.39 ± 0.31; DCM 1.72 ± 0.69; NC 2.91 ± 0.78). Mean peripheral perfusion also increased but not significantly and accompanied with great variations within and between groups (mean PPR: CAD 1.30 ± 0.79; SX 1.36 ± 0.71; DCM 1.60 ± 1.22; NC 1.27 ± 0.63). The mean difference between PPR and MPR for all subpopulations varied widely. No significant correlations in flow reserve were found between peripheral and myocardial microcirculatory beds in any of the groups (Total group: r = -0.07, SEE = 0.70, CAD: r = 0.14, SEE = 0.48, SX: r = 0.17, SEE = 0.30, DCM: r = -0.11, SEE = 0.71, NC: r = -0.19, SEE = 0.80).
No correlations between myocardial and peripheral perfusion (reserve) were found in different patient populations in the same PET session. This suggests a functional difference between peripheral and myocardial flow in the response to intravenously administered adenosine stress.
[13N]氨正电子发射断层扫描(PET)可用于定量评估心肌灌注。外周血流量与心肌灌注量之间的相似性尚不清楚。我们比较了静息和腺苷应激状态下[13N]氨心肌灌注 PET 扫描中心肌与上肢的灌注流量,以确定外周灌注储备(PPR)是否与 MPR 相关。
对 58 例患者(27 例男性,31 例女性,年龄 64±13 岁)进行了[13N]氨心肌灌注 PET 扫描评估,并分为 4 组:冠心病(CAD)患者 15 例,心脏综合征 X(SX)患者 14 例,特发性扩张型心肌病(DCM)患者 16 例,和正常对照组(NC)患者 13 例。通过双组织室模型测量上肢近端肌肉组织的外周肢体灌注,并对其进行量化,同时计算 PPR(应激/休息比值)。通过双组织室模型计算 MPR。比较 PPR 结果与 MPR 结果。
所有组的心肌灌注均显著增加,表现为 MPR 增加(CAD:1.99±0.47;SX:1.39±0.31;DCM:1.72±0.69;NC:2.91±0.78)。外周灌注也增加,但无统计学意义,且组内和组间变化较大(平均 PPR:CAD:1.30±0.79;SX:1.36±0.71;DCM:1.60±1.22;NC:1.27±0.63)。所有亚群的 PPR 与 MPR 之间的平均差值差异很大。在任何组中,外周和心肌微循环之间的血流储备均无显著相关性(总组:r=-0.07,SEE=0.70,CAD:r=0.14,SEE=0.48,SX:r=0.17,SEE=0.30,DCM:r=-0.11,SEE=0.71,NC:r=-0.19,SEE=0.80)。
在同一 PET 检查中,不同患者群体的心肌与外周灌注(储备)之间未见相关性。这表明在外周和心肌血流对静脉内给予腺苷的应激反应方面存在功能差异。