Centro de Evidências em Oncologia, Universidade Estadual de Campinas, São Paulo, Brazil.
BMC Cancer. 2011 Mar 31;11:115. doi: 10.1186/1471-2407-11-115.
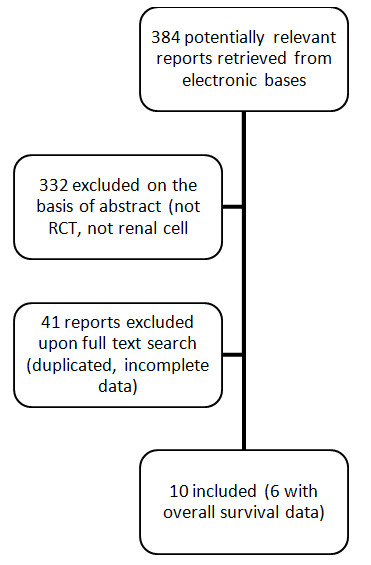
Many adjuvant trials have been undertaken in an attempt to reduce the risk of recurrence among patients who undergo surgical resection for locally advanced renal cancer. However, no clear benefit has been identified to date. This systematic review was conducted to examine the exact role of adjuvant therapy in renal cancer setting.
Randomized controlled trials were searched comparing adjuvant therapy (chemotherapy, vaccine, immunotherapy, biochemotherapy) versus no active treatment after surgery among renal cell cancer patients. Outcomes were overall survival (OS), disease-free survival (DFS), and severe toxicities. Risk ratios (RR), hazard ratios (HR) and 95% confidence intervals were calculated using a fixed-effects meta-analysis. Heterogeneity was measured by I2. Different strategies of adjuvant treatment were evaluated separately.
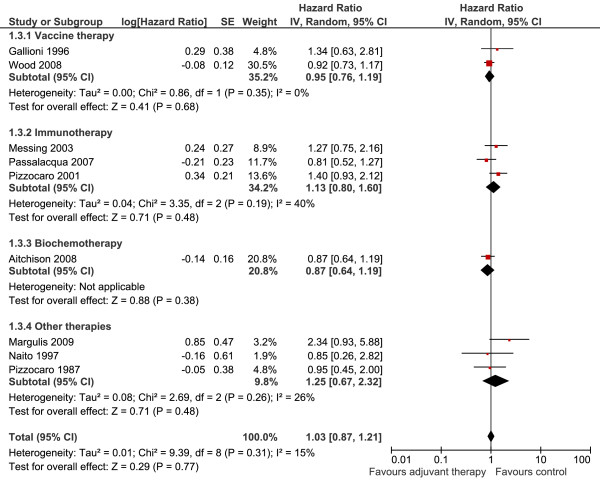
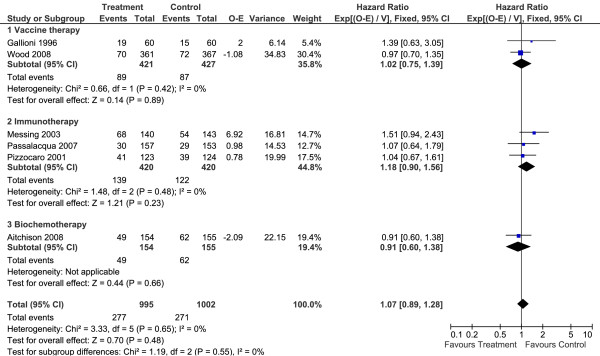
Ten studies (2,609 patients) were included. Adjuvant therapy provided no benefits in terms of OS (HR 1.07; 95%CI 0.89 to 1.28; P = 0.48 I2 = 0%) or DFS (HR 1.03; 95%CI 0.87 to 1.21; P = 0.77 I2 = 15%) when compared to no treatment. No subgroup analysis (immunotherapy, vaccines, biochemotherapy and hormone therapy) had relevant results. Toxicity evaluation depicted a significantly higher frequency of serious adverse events in the adjuvant group.
This analysis provided no support for the hypothesis that the agents studied provide any clinical benefit for renal cancer patients although they increase the risk of toxic effects. Randomized trials are underway to test targeted therapies, which might open a new therapeutic frontier. Until these trials yield results, no adjuvant therapy can be recommended for patients who undergo surgical resection for renal cell cancer.
许多辅助治疗试验已经进行,试图降低接受手术切除局部晚期肾细胞癌的患者的复发风险。然而,迄今为止尚未确定明确的获益。本系统评价旨在检查辅助治疗在肾细胞癌治疗中的确切作用。
搜索了比较辅助治疗(化疗、疫苗、免疫治疗、生物化疗)与手术后无积极治疗的随机对照试验,纳入肾细胞癌患者。主要研究终点为总生存期(OS)、无病生存期(DFS)和严重毒性。使用固定效应荟萃分析计算风险比(RR)、风险比(HR)和 95%置信区间。使用 I2 测量异质性。分别评估了不同的辅助治疗策略。
共纳入 10 项研究(2609 例患者)。与无治疗相比,辅助治疗并未带来 OS(HR 1.07;95%CI 0.89 至 1.28;P = 0.48 I2 = 0%)或 DFS(HR 1.03;95%CI 0.87 至 1.21;P = 0.77 I2 = 15%)的获益。免疫治疗、疫苗、生物化疗和激素治疗等亚组分析均无相关结果。毒性评估显示辅助组严重不良事件的发生频率显著增加。
本分析不支持所研究的药物为肾细胞癌患者提供任何临床获益的假设,尽管它们增加了毒副作用的风险。目前正在进行针对靶向治疗的随机试验,这可能为治疗开辟新的前沿。在这些试验产生结果之前,不能推荐辅助治疗用于接受手术切除的肾细胞癌患者。