Fiocca F, Donatelli G, Ceci V, Cereatti F, Romagnoli F, Simonelli L, Modini C
Department of Emergency and Urgency, Policlinico Umberto I, University, 'La Sapienza', Rome, Italy.
Case Rep Gastroenterol. 2008 Mar 14;2(1):116-20. doi: 10.1159/000119713.
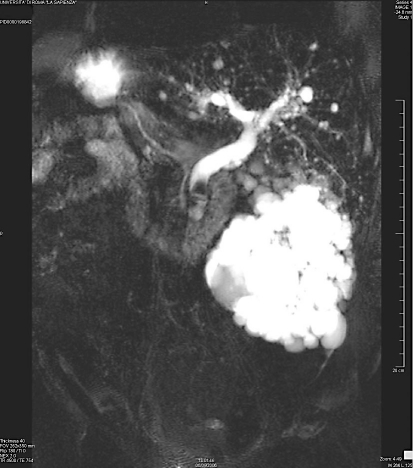
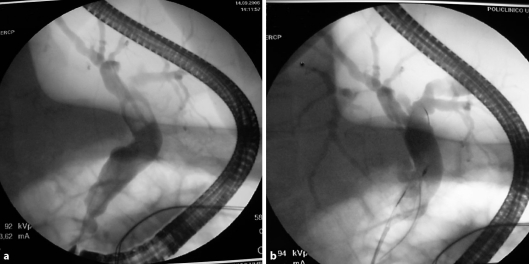
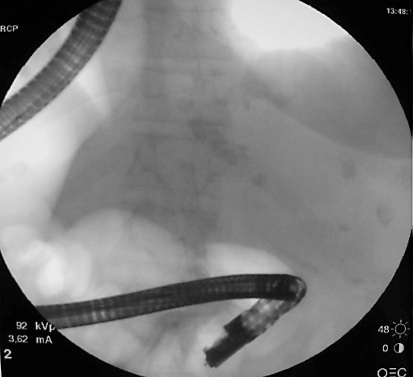
A 69-year-old cholecystectomized female with known total situs viscerum inversus presented recurrent colicky pain in the left upper abdominal quadrant and jaundice. Laboratory parameters showed increased neutrophils and coniugated bilirubin of 5.53 mg/dl. US and MRCP confirmed total situs viscerum inversus and a dilatation of the intra- and extrahepatic ducts with a peripapillary 13 mm stone. ERCP, sphincterotomy and successful common bile duct stone extraction were performed in the conventional way. ERCP was carried out successfully despite situs inversus maintaining the patient in the prone position with the endoscopist on the right side of the table. Some authors have reported similar cases in whom ERCP was performed in other positions, while this report shows that an experienced endoscopist can achieve the same results in the conventional way as it is possible when anatomical changes, Billroth II or Roux-en-Y, or different positions of the patient, supine or on the left side, are present.
一名69岁的女性,已知患有完全性内脏反位,曾接受胆囊切除术,现左上腹反复出现绞痛并伴有黄疸。实验室检查参数显示中性粒细胞增多,结合胆红素为5.53mg/dl。超声和磁共振胰胆管造影(MRCP)证实为完全性内脏反位,肝内和肝外胆管扩张,伴有一个乳头周围13mm的结石。通过传统方法进行了内镜逆行胰胆管造影(ERCP)、括约肌切开术并成功取出胆总管结石。尽管存在内脏反位,仍成功进行了ERCP,将患者置于俯卧位,内镜医师位于手术台右侧。一些作者报道过在其他体位进行ERCP的类似病例,而本报告表明,经验丰富的内镜医师采用传统方法能够取得与存在解剖结构改变、毕罗Ⅱ式或 Roux-en-Y吻合术,或患者处于仰卧位或左侧卧位等不同情况时相同的结果。