Department of Surgery, McGill University, Montreal, QC H3A1A1, Canada.
World J Surg Oncol. 2011 Apr 14;9:40. doi: 10.1186/1477-7819-9-40.
Thick melanomas (TM) ≥4 mm have a high risk for nodal and distant metastases. Optimal surgical management, prognostic significance of sentinel node biopsy (SLNB), and benefits of interferon (IFN) for these patients are unclear. As a continuum of increasing tumor thickness is placed into a single TM group, differences in biologic and clinical behavior may be lost. The purpose of this study was to better characterize the diverse biology in TM, including the value of increasing thickness and nodal status information, potentially identifying high risk TM subgroups that may warrant more aggressive treatment/follow up.
155 consecutive TM patients treated at a single institution between 1971 and 2007 were retrospectively reviewed. Patient, disease and treatment features were analyzed with respect to disease-free (DFS) and overall survival (OS).
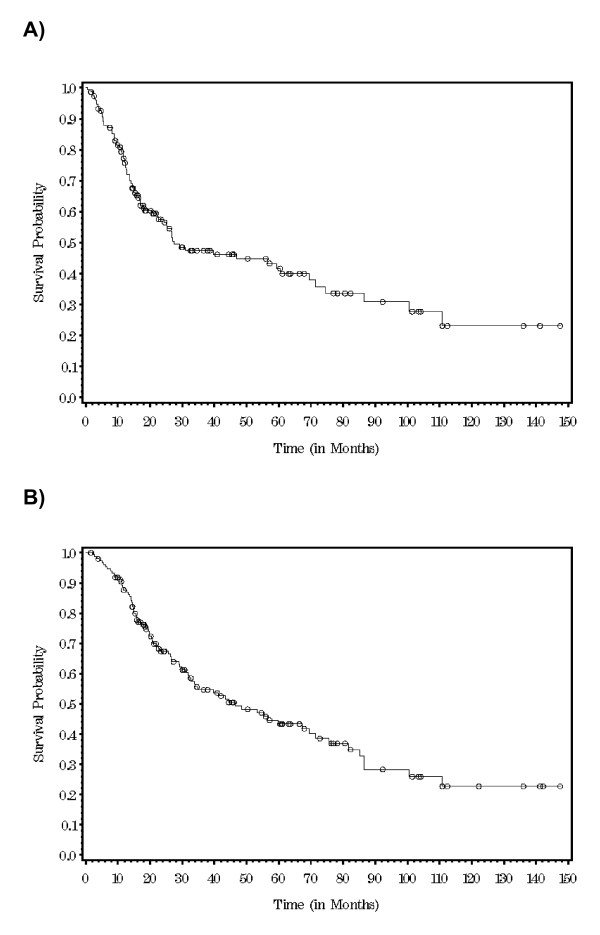
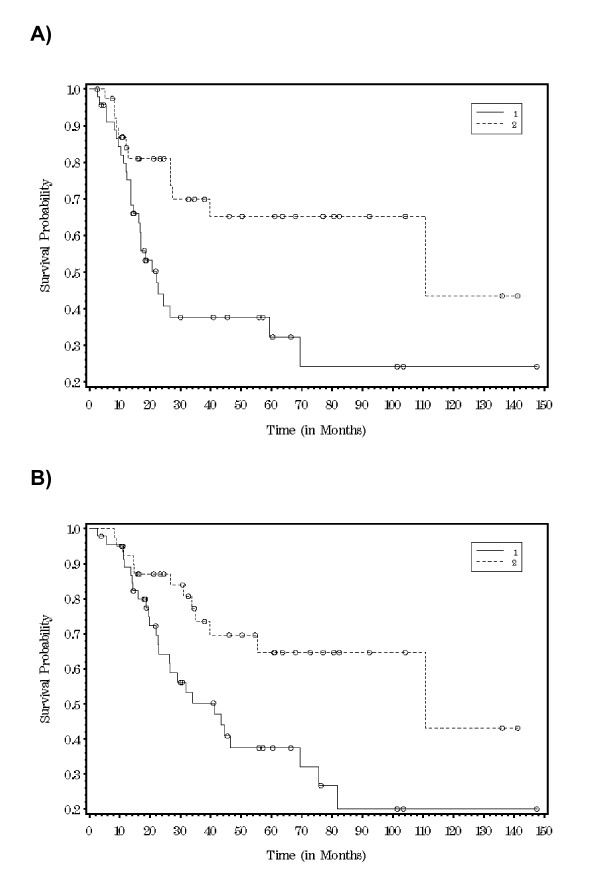
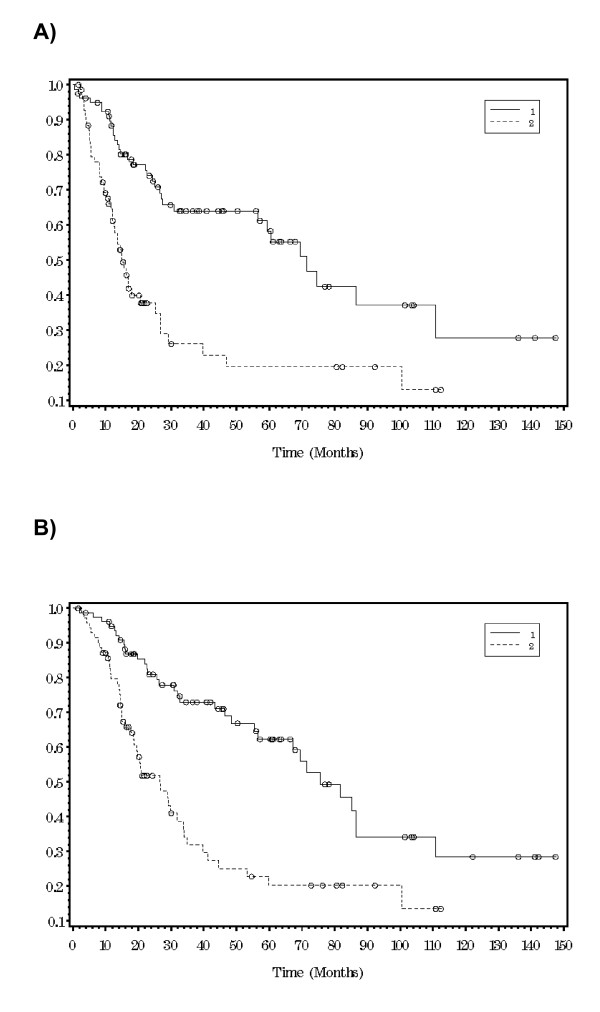
Median patient age was 66 years and 68% of patients were men. The trunk was the most common TM location (35%), followed by the head and neck (29%) and lower extremities (20%). Median thickness was 6 mm and 61% were ulcerated. 6% patients had stage IV disease, 12% had clinical nodal metastases. Clinically negative lymph node basins were treated by observation (22 patients--15.4%), elective lymph node dissection (ELND) (24 patients--17.6%) or SLNB (91 patients--67%). 75% of ELND's and 53% of SLNB's were positive. Completion node dissection was performed in 38 SLNB+ patients and 22% had additional positive nodes. 17% of the study patients received IFN. At median follow up of 26 months, 5 year DFS and OS were 42% and 43.6%. For SLNB positive vs negative, median DFS were 22 vs 111 months (p = 0.006) and median OS were 41 vs 111 months (p = 0.006). When stratified by tumor thickness ≤ vs > 6 mm, 5 year DFS was 58.3% vs 20% (p < 0.0001) and OS was 62% vs 20% (P < 0.0001). IFN had no impact on DFS or OS (p = 0.98 and 0.8 respectively).
Within the high risk group of patients with TM, cases with tumor thickness > 6 mm or a positive SLNB had a significantly worse DFS and OS (p < .0001, <.0001 and .006, .006).
厚度大于 4 毫米的黑色素瘤(TM)有发生淋巴结和远处转移的高风险。最佳的手术管理、前哨淋巴结活检(SLNB)的预后意义以及干扰素(IFN)对这些患者的益处尚不清楚。由于不断增加的肿瘤厚度被归入单一的 TM 组,因此其生物学和临床行为的差异可能会丢失。本研究的目的是更好地描述 TM 中不同的生物学特性,包括厚度增加和淋巴结状态信息的价值,从而有可能确定可能需要更积极治疗/随访的高危 TM 亚组。
回顾性分析了 1971 年至 2007 年期间在一家机构接受治疗的 155 例连续 TM 患者。分析了患者、疾病和治疗特征与无病生存(DFS)和总生存(OS)的关系。
中位患者年龄为 66 岁,68%的患者为男性。最常见的 TM 部位是躯干(35%),其次是头颈部(29%)和下肢(20%)。中位厚度为 6 毫米,61%为溃疡。6%的患者有 IV 期疾病,12%有临床淋巴结转移。临床阴性淋巴结盆接受观察(22 例,15.4%)、选择性淋巴结清扫术(ELND,24 例,17.6%)或 SLNB(91 例,67%)治疗。ELND 的 75%和 SLNB 的 53%为阳性。38 例 SLNB+患者进行了完全淋巴结清扫术,其中 22%有额外的阳性淋巴结。17%的研究患者接受了 IFN 治疗。在中位随访 26 个月时,5 年 DFS 和 OS 分别为 42%和 43.6%。对于 SLNB 阳性与阴性,中位 DFS 分别为 22 个月与 111 个月(p=0.006),中位 OS 分别为 41 个月与 111 个月(p=0.006)。当按肿瘤厚度≤6 毫米与>6 毫米分层时,5 年 DFS 分别为 58.3%与 20%(p<0.0001),OS 分别为 62%与 20%(P<0.0001)。IFN 对 DFS 或 OS 没有影响(p=0.98 和 0.8)。
在 TM 高危患者中,肿瘤厚度>6 毫米或 SLNB 阳性的患者 DFS 和 OS 显著更差(p<0.0001,<0.0001 和<.0001,.006 和.006)。