Castelnuovo Barbara, Sempa Joseph, Agnes Kiragga N, Kamya Moses R, Manabe Yukari C
Infectious Diseases Institute, Makerere University, Mulago Hospital Complex, P.O. Box 22418, Kampala, Uganda.
AIDS Res Treat. 2011;2011:736938. doi: 10.1155/2011/736938. Epub 2011 Apr 10.
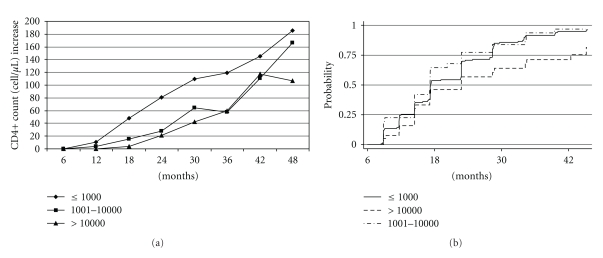
Our objective was to evaluate outcomes in patients with sustained viral suppression compared to those with episodes of viremia. Methods. In a prospective cohort of patients started on ART in Uganda and followed for 48 months, patients were categorized according to viral load (VL): (1) sustained-suppression: (VL ≤1,000 copies/mL) (2) VL 1,001-10,000, or (3) VL >10,000. Results. Fifty-Three (11.2%) and 84 (17.8%) patients had a first episode of intermediate and high viremia, respectively. Patients with sustained suppression had better CD4+ T cell count increases over time compared to viremic patients (P < .001). The majority of patients with viremia achieved viral suppression when the measurement was repeated. Only 39.6% of patients with intermediate and 19.1% with high viremia eventually needed to be switched to second line (P = .008). Conclusions. The use of at least one repeat measurement rather than a single VL measurement could avert from 60% to 80% of unnecessary switches.
我们的目标是评估与病毒血症发作患者相比,病毒持续抑制患者的治疗结果。方法。在乌干达开始接受抗逆转录病毒治疗(ART)并随访48个月的前瞻性队列患者中,根据病毒载量(VL)对患者进行分类:(1)持续抑制:(VL≤1000拷贝/毫升)(2)VL为1001 - 10000,或(3)VL>10000。结果。分别有53例(11.2%)和84例(17.8%)患者首次出现中度和高度病毒血症。与病毒血症患者相比,持续抑制的患者随着时间推移CD4 + T细胞计数增加得更好(P <.001)。重复测量时,大多数病毒血症患者实现了病毒抑制。最终只有39.6%的中度病毒血症患者和19.1%的高度病毒血症患者需要换用二线治疗(P =.008)。结论。使用至少一次重复测量而非单次VL测量可避免60%至80%的不必要换药。