McGrail Kimberlyn M
Open Med. 2008;2(4):e91-8. Epub 2008 Oct 21.
The primary demonstration of the principle of income-related equity in Canada is the provision of health care services based on need rather than ability to pay. Despite this principle, Canada, along with other OECD countries, exhibits income-related variations in the use of health care services. This paper extends previous analyses to include surgical day care, assesses changes in income-related equity between 1992 and 2002 in British Columbia and tests the feasibility of using administrative data for general equity analyses.
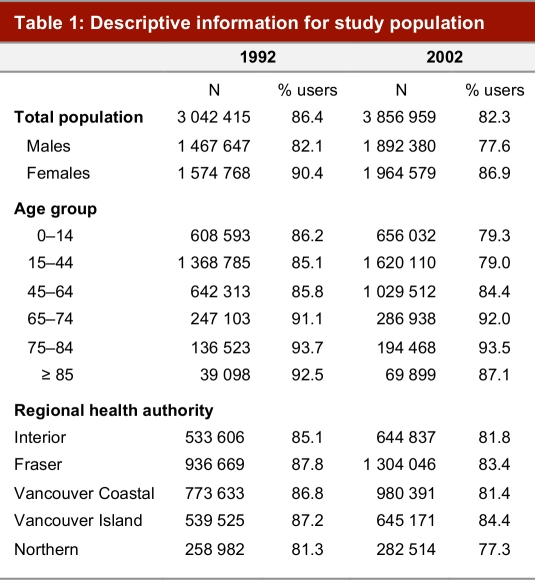
Data derive from the BC Linked Health Database and from a custom tabulation of income tax filer data provided by Statistics Canada. Cross-sectional analyses measure inequity in the probability and conditional use of services using concentration indices, which summarize health care services use for individuals ranked by income, after standardization for age, sex, region of residence and need for health care services.
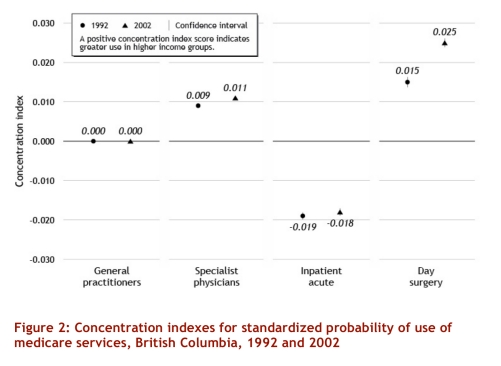
Small but systematic relationships were found between income and use of health care services for all types of services, with the exception of visits to general practitioners (GPs). Lower income is associated with greater conditional use of GPs and greater use of acute inpatient care. Higher income is associated with the greater use of specialist and surgical day care services; the latter inequity was found to grow substantially over time.
Deviations from equity deserve further investigation, especially because the use of day care surgery is continually expanding. For example, an understanding of the reasons for differential admission rates to acute and day surgery might provide insight as to whether community-based services could help shift some acute care use among lower income groups to surgical day care. It is possible to use administrative data to monitor income-related equity, and future research should take advantage of this possibility.
加拿大与收入相关的公平原则的主要体现是根据需求而非支付能力提供医疗保健服务。尽管有这一原则,但加拿大与其他经合组织国家一样,在医疗保健服务的使用方面存在与收入相关的差异。本文扩展了先前的分析,将日间手术护理纳入其中,评估了1992年至2002年不列颠哥伦比亚省与收入相关的公平性变化,并测试了使用行政数据进行总体公平性分析的可行性。
数据来源于不列颠哥伦比亚省关联健康数据库以及加拿大统计局提供的所得税申报者数据的定制列表。横断面分析使用集中度指数衡量服务使用概率和条件使用方面的不公平性,该指数在对年龄、性别、居住地区和医疗保健服务需求进行标准化后,总结了按收入排名的个人的医疗保健服务使用情况。
除了全科医生(GP)就诊外,在所有类型的服务中都发现了收入与医疗保健服务使用之间存在微小但系统的关系。低收入与更多地有条件使用全科医生以及更多地使用急性住院护理相关。高收入与更多地使用专科和日间手术护理服务相关;发现后者的不公平性随着时间的推移大幅增加。
与公平性的偏差值得进一步研究,特别是因为日间手术护理的使用在不断扩大。例如,了解急性手术和日间手术不同入院率的原因,可能有助于洞察基于社区的服务是否可以帮助将低收入群体中的一些急性护理使用转移到日间手术护理。利用行政数据监测与收入相关的公平性是可行的,未来的研究应利用这一可能性。