Kenya Medical Research Institute-Wellcome Trust Research Programme, P,O Box 230, Kilifi, Kenya.
Int J Equity Health. 2011 May 26;10:22. doi: 10.1186/1475-9276-10-22.
Equity and universal coverage currently dominate policy debates worldwide. Health financing approaches are central to universal coverage. The way funds are collected, pooled, and used to purchase or provide services should be carefully considered to ensure that population needs are addressed under a universal health system. The aim of this paper is to assess the extent to which the Kenyan health financing system meets the key requirements for universal coverage, including income and risk cross-subsidisation. Recommendations on how to address existing equity challenges and progress towards universal coverage are made.
An extensive review of published and gray literature was conducted to identify the sources of health care funds in Kenya. Documents were mainly sourced from the Ministry of Medical Services and the Ministry of Public Health and Sanitation. Country level documents were the main sources of data. In cases where data were not available at the country level, they were sought from the World Health Organisation website. Each financing mechanism was analysed in respect to key functions namely, revenue generation, pooling and purchasing.
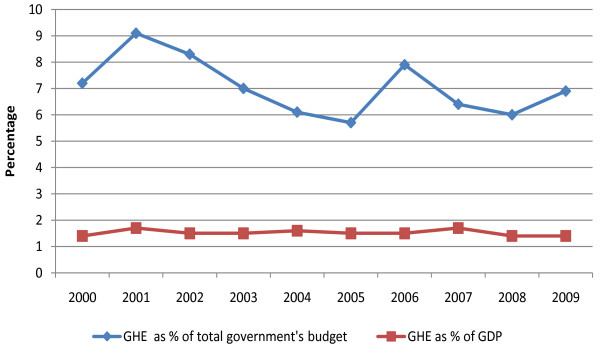
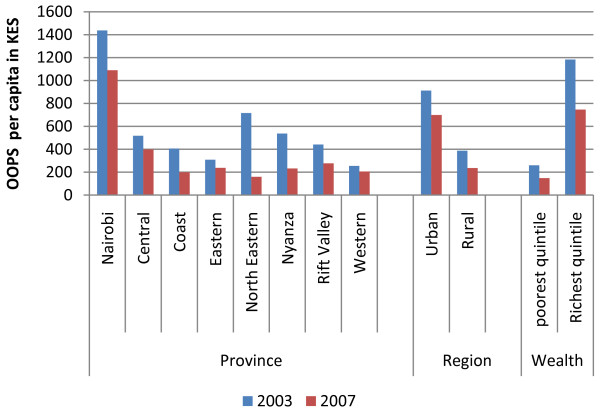
The Kenyan health sector relies heavily on out-of-pocket payments. Government funds are mainly allocated through historical incremental approach. The sector is largely underfunded and health care contributions are regressive (i.e. the poor contribute a larger proportion of their income to health care than the rich). Health financing in Kenya is fragmented and there is very limited risk and income cross-subsidisation. The country has made little progress towards achieving international benchmarks including the Abuja target of allocating 15% of government's budget to the health sector.
The Kenyan health system is highly inequitable and policies aimed at promoting equity and addressing the needs of the poor and vulnerable have not been successful. Some progress has been made towards addressing equity challenges, but universal coverage will not be achieved unless the country adopts a systemic approach to health financing reforms. Such an approach should be informed by the wider health system goals of equity and efficiency.
公平性和全民覆盖目前主导着全球范围内的政策辩论。卫生筹资方法是全民覆盖的核心。资金的筹集、汇集和用于购买或提供服务的方式应仔细考虑,以确保在全民健康系统下满足人口的需求。本文旨在评估肯尼亚卫生筹资系统在多大程度上满足全民覆盖的关键要求,包括收入和风险的交叉补贴。就如何解决现有公平性挑战以及在全民覆盖方面取得进展提出了建议。
对已发表和灰色文献进行了广泛的审查,以确定肯尼亚卫生保健资金的来源。文件主要来自医疗服务部和公共卫生与卫生署。国家一级的文件是数据的主要来源。在国家一级没有数据的情况下,从世界卫生组织的网站上获取数据。对每个筹资机制进行了分析,涉及关键职能,即收入的产生、汇集和采购。
肯尼亚卫生部门严重依赖自费支付。政府资金主要通过历史递增方法分配。该部门资金严重短缺,卫生保健缴款呈倒退趋势(即穷人用于卫生保健的收入比例高于富人)。肯尼亚的卫生筹资分散,风险和收入的交叉补贴非常有限。该国在实现国际基准方面进展甚微,包括阿布贾目标,即将政府预算的 15%分配给卫生部门。
肯尼亚的卫生系统极不公平,旨在促进公平和满足穷人和弱势群体需求的政策并未取得成功。在解决公平性挑战方面取得了一些进展,但除非该国采取系统性的卫生筹资改革方法,否则无法实现全民覆盖。这种方法应该以更广泛的卫生系统公平和效率目标为指导。