Department of Radiation Oncology, The University of Texas M. D. Anderson Cancer Center, Houston, Texas, USA.
Cancer. 2011 Jun 15;117(12):2754-61. doi: 10.1002/cncr.25823. Epub 2010 Dec 14.
A study was undertaken to assess patient navigation utilization and its impact on treatment interruptions and clinical trial enrollment among American Indian cancer patients.
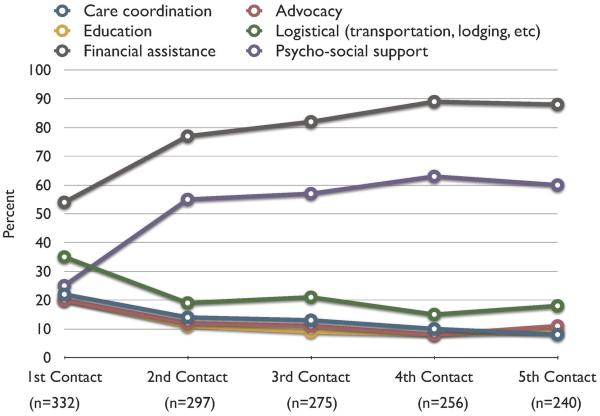
Between February 2004 and September 2009, 332 American Indian cancer patients received patient navigation services throughout cancer treatment. The patient navigation program provided culturally competent navigators to assist patients with navigating cancer therapy, obtaining medications, insurance issues, communicating with medical providers, and travel and lodging logistics. Data on utilization and trial enrollment were prospectively collected. Data for a historical control group of 70 American Indian patients who did not receive patient navigation services were used to compare treatment interruptions among those undergoing patient navigation during curative radiation therapy (subgroup of 123 patients).
The median number of contacts with a navigator was 12 (range, 1-119). The median time spent with the navigator at first contact was 40 minutes (range, 10-250 minutes), and it was 15 minutes for subsequent contacts. Patients treated with radiation therapy with curative intent who underwent patient navigation had fewer days of treatment interruption (mean, 1.7 days; 95% confidence interval [CI], 1.1-2.2 days) than historical controls who did not receive patient navigation services (mean, 4.9 days; 95% CI, 2.9-6.9 days). Of the 332 patients, 72 (22%; 95% CI, 17%-26%) were enrolled on a clinical treatment trial or cancer control protocol.
Patient navigation was associated with fewer treatment interruptions and relatively high rates of clinical trial enrollment among American Indian cancer patients compared with national reports.
本研究旨在评估美国印第安癌症患者中患者导航的使用情况及其对治疗中断和临床试验入组的影响。
2004 年 2 月至 2009 年 9 月期间,332 名美国印第安癌症患者在整个癌症治疗过程中接受了患者导航服务。患者导航计划提供了具有文化能力的导航员,以帮助患者进行癌症治疗、获取药物、解决保险问题、与医疗服务提供者沟通以及处理旅行和住宿后勤问题。前瞻性收集了利用和试验登记数据。利用未接受患者导航服务的 70 名美国印第安患者的历史对照数据来比较接受患者导航治疗的患者(123 名患者的亚组)在接受根治性放射治疗期间的治疗中断情况。
导航员的平均联系次数为 12 次(范围 1-119)。首次与导航员联系时,平均花费 40 分钟(范围 10-250 分钟),后续联系则为 15 分钟。接受根治性放疗的患者接受患者导航治疗的中断天数(平均 1.7 天;95%置信区间 [CI],1.1-2.2 天)明显少于未接受患者导航服务的历史对照患者(平均 4.9 天;95%CI,2.9-6.9 天)。在 332 名患者中,有 72 名(22%;95%CI,17%-26%)患者入组了临床治疗试验或癌症控制方案。
与全国报告相比,患者导航与美国印第安癌症患者的治疗中断减少和临床试验入组率相对较高相关。