Banerjee Dipanjan, Wong Eric C, Shin Jessica, Fortmann Stephen P, Palaniappan Latha
Program on Prevention Outcomes and Practices, Stanford Prevention Research Center, Stanford University School of Medicine, Stanford, CA 94305, USA.
J Lipids. 2011;2011:291954. doi: 10.1155/2011/291954. Epub 2011 May 23.
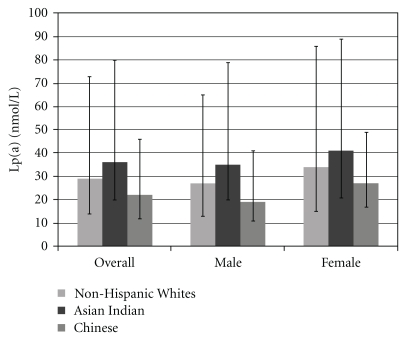
Background. Lipoprotein (a) [Lp(a)] is an independent risk factor for cardiovascular disease (CVD) in Non-Hispanic Whites (NHW). There are known racial/ethnic differences in Lp(a) levels, and the association of Lp(a) with CVD outcomes has not been examined in Asian Americans in the USA. Objective. We hypothesized that Lp(a) levels would differ in Asian Indians and Chinese Americans when compared to NHW and that the relationship between Lp(a) and CVD outcomes would be different in these Asian racial/ethnic subgroups when compared to NHW. Methods. We studied the outpatient electronic health records of 2022 NHW, 295 Asian Indians, and 151 Chinese adults age ≥18 y in Northern California in whom Lp(a) levels were assessed during routine clinical care from 2001 to 2008, excluding those who had received prescriptions for niacin (14.6%). Nonparametric methods were used to compare median Lp(a) levels. Significance was assessed at the P < .0001 level to account for multiple comparisons. CVD outcomes were defined as ischemic heart disease (IHD) (265 events), stroke (122), or peripheral vascular disease (PVD) (87). We used logistic regression to determine the relationship between Lp(a) and CVD outcomes. Results. Both Asian Indians (36 nmol/L) and NHW (29 nmol/L) had higher median Lp(a) levels than Chinese (22 nmol/L, P ≤ .0001 and P = .0032). When stratified by sex, the differences in median Lp(a) between these groups persisted in the 1761 men (AI v CH: P = .001, NHW v CH: P = .0018) but were not statistically significant in the 1130 women (AI v CH: P = .0402, NHW v CH: P = .0761). Asian Indians (OR = 2.0) and Chinese (OR = 4.8) exhibited a trend towards greater risk of IHD with high Lp(a) levels than NHW (OR = 1.4), but no relationship was statistically significant. Conclusion. Asian Indian and NHW men have higher Lp(a) values than Chinese men, with a trend toward, similar associations in women. High Lp(a) may be more strongly associated with IHD in Asian Indians and Chinese, although we did not have a sufficient number of outcomes to confirm this. Further studies should strive to elucidate the relationship between Lp(a) levels, CVD, and race/ethnicity among Asian subgroups in the USA.
背景。脂蛋白(a)[Lp(a)]是非西班牙裔白人(NHW)心血管疾病(CVD)的独立危险因素。已知Lp(a)水平存在种族/民族差异,在美国亚裔美国人中尚未研究Lp(a)与CVD结局的关联。目的。我们假设,与NHW相比,亚洲印度人和华裔美国人的Lp(a)水平会有所不同,并且与NHW相比,这些亚洲种族/民族亚组中Lp(a)与CVD结局之间的关系也会有所不同。方法。我们研究了北加利福尼亚州2022名NHW、295名亚洲印度人和151名年龄≥18岁的华裔成年人的门诊电子健康记录,这些人在2001年至2008年的常规临床护理期间接受了Lp(a)水平评估,排除了那些接受过烟酸处方的人(14.6%)。采用非参数方法比较Lp(a)水平中位数。为了考虑多重比较,在P <.0001水平评估显著性。CVD结局定义为缺血性心脏病(IHD)(265例事件)、中风(122例)或外周血管疾病(PVD)(87例)。我们使用逻辑回归来确定Lp(a)与CVD结局之间的关系。结果。亚洲印度人(36 nmol/L)和NHW(29 nmol/L)的Lp(a)水平中位数均高于华裔(22 nmol/L,P≤.0001和P =.0032)。按性别分层时,这些组之间Lp(a)中位数的差异在1761名男性中持续存在(亚洲印度人与华裔:P =.001,NHW与华裔:P =.0018),但在1130名女性中无统计学意义(亚洲印度人与华裔:P =.0402,NHW与华裔:P =.0761)。亚洲印度人(OR = 2.0)和华裔(OR = 4.8)与NHW(OR = 1.4)相比,Lp(a)水平高时患IHD的风险有增加趋势,但无统计学意义。结论。亚洲印度男性和NHW男性的Lp(a)值高于华裔男性,女性中也有类似关联趋势。高Lp(a)可能与亚洲印度人和华裔的IHD关联更强,尽管我们没有足够数量的结局来证实这一点。进一步的研究应努力阐明美国亚洲亚组中Lp(a)水平、CVD与种族/民族之间的关系。