Center for Integrated Health Care Research, Kaiser Permanente Hawai'i, Honolulu, HI, USA.
Stanford University School of Medicine, Stanford, CA, USA.
BMC Public Health. 2023 May 15;23(1):885. doi: 10.1186/s12889-023-15795-5.
Cardiovascular disease (CVD) remains the leading cause of death in the US. CVD incidence is influenced by many demographic, clinical, cultural, and psychosocial factors, including race and ethnicity. Despite recent research, there remain limitations on understanding CVD health among Asians and Pacific Islanders (APIs), particularly some subgroups and multi-racial populations. Combining diverse API populations into one study group and difficulties in defining API subpopulations and multi-race individuals have hampered efforts to identify and address health disparities in these growing populations.
The study cohort was comprised of all adult patients at Kaiser Permanente Hawai'i and Palo Alto Medical Foundation in California during 2014-2018 (n = 684,363). EHR-recorded ICD-9 and ICD-10 diagnosis codes were used to indicate coronary heart disease (CHD), stroke, peripheral vascular disease (PVD), and overall CVD. Self-reported race and ethnicity data were used to construct 12 mutually exclusive single and multi-race groups, and a Non-Hispanic White (NHW) comparison group. Logistic regression models were used to derive prevalence estimates, odds ratios, and confidence intervals for the 12 race/ethnicity groups.
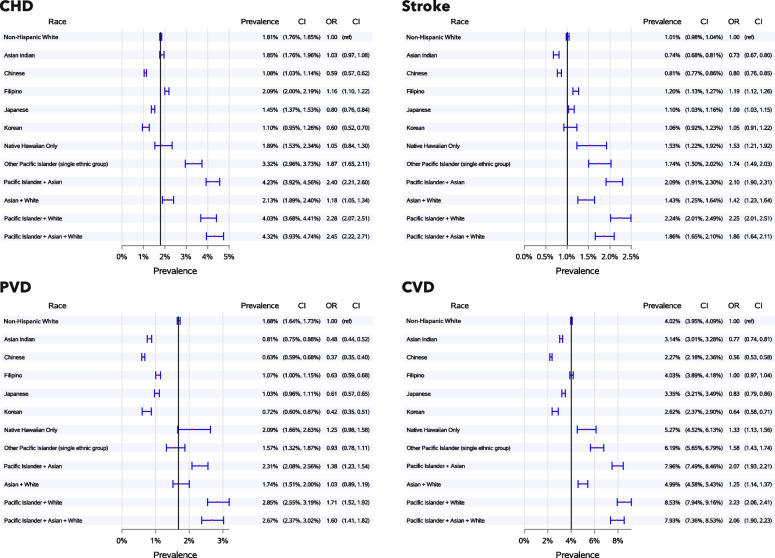
The prevalence of CHD and PVD varied 4-fold and stroke and overall CVD prevalence varied 3-fold across API subpopulations. Among Asians, the Filipino subgroup had the highest prevalence of all three CVD conditions and overall CVD. Chinese people had the lowest prevalence of CHD, PVD and overall CVD. In comparison to Native Hawaiians, Other Pacific Islanders had significantly higher prevalence of CHD. For the multi-race groups that included Native Hawaiians and Other Pacific Islanders, the prevalence of overall CVD was significantly higher than that for either single-race Native Hawaiians or Other Pacific Islanders. The multi-race Asian + White group had significantly higher overall CVD prevalence than both the NHW group and the highest Asian subgroup (Filipinos).
Study findings revealed significant differences in overall CVD, CHD, stroke, and PVD among API subgroups. In addition to elevated risk among Filipino, Native Hawaiian, and Other Pacific Islander groups, the study identified particularly elevated risk among multi-race API groups. Differences in disease prevalence are likely mirrored in other cardiometabolic conditions, supporting the need to disaggregate API subgroups in health research.
心血管疾病(CVD)仍然是美国的主要死亡原因。CVD 的发病率受到许多人口统计学、临床、文化和社会心理因素的影响,包括种族和民族。尽管最近进行了研究,但对于亚洲人和太平洋岛民(APIs)的 CVD 健康状况仍存在理解上的局限性,特别是一些亚群和多种族人群。将不同的 API 人群合并到一个研究组中,以及在定义 API 亚群和多种族个体方面的困难,阻碍了在这些不断增长的人群中识别和解决健康差异的努力。
研究队列包括 2014 年至 2018 年期间在 Kaiser Permanente 夏威夷和加利福尼亚州的 Palo Alto Medical Foundation 的所有成年患者(n=684363)。使用电子病历记录的 ICD-9 和 ICD-10 诊断代码来表示冠心病(CHD)、中风、外周血管疾病(PVD)和总体 CVD。使用自我报告的种族和民族数据构建了 12 个相互排斥的单一和多种族群体,以及一个非西班牙裔白人(NHW)对照组。使用逻辑回归模型得出 12 个种族/民族群体的患病率估计、优势比和置信区间。
在 API 亚群中,CHD 和 PVD 的患病率相差 4 倍,中风和总体 CVD 的患病率相差 3 倍。在亚洲人中,菲律宾亚群的所有三种 CVD 疾病和总体 CVD 的患病率最高。中国人的 CHD、PVD 和总体 CVD 的患病率最低。与夏威夷原住民相比,其他太平洋岛民的 CHD 患病率明显更高。对于包括夏威夷原住民和其他太平洋岛民的多种族群体,总体 CVD 的患病率明显高于单一族裔的夏威夷原住民或其他太平洋岛民。多种族的亚洲+白人组的总体 CVD 患病率明显高于 NHW 组和最高的亚洲亚组(菲律宾人)。
研究结果显示,API 亚群的总体 CVD、CHD、中风和 PVD 存在显著差异。除了菲律宾人、夏威夷原住民和其他太平洋岛民群体的风险升高外,该研究还发现多种族 API 群体的风险特别高。疾病患病率的差异可能反映在其他心血管代谢疾病中,支持在健康研究中对 API 亚群进行细分的必要性。