The Research Department & Paediatric Ward, Hillerød Hospital, Denmark.
BMC Pediatr. 2011 Jun 14;11:55. doi: 10.1186/1471-2431-11-55.
Adolescents with type 1 diabetes face demanding challenges due to conflicting priorities between psychosocial needs and diabetes management. This conflict often results in poor glycaemic control and discord between adolescents and parents. Adolescent-parent conflicts are thus a barrier for health care providers (HCPs) to overcome in their attempts to involve both adolescents and parents in improvement of glycaemic control. Evidence-based interventions that involve all three parties (i.e., adolescents, parents and HCPs) and are integrated into routine outpatient clinic visits are lacking. The Guided Self-Determination method is proven effective in adult care and has been adapted to adolescents and parents (Guided Self-Determination-Young (GSD-Y)) for use in paediatric diabetes outpatient clinics. Our objective is to test whether GSD-Y used in routine paediatric outpatient clinic visits will reduce haemoglobin A1c (HbA1c) concentrations and improve adolescents' life skills compared with a control group.
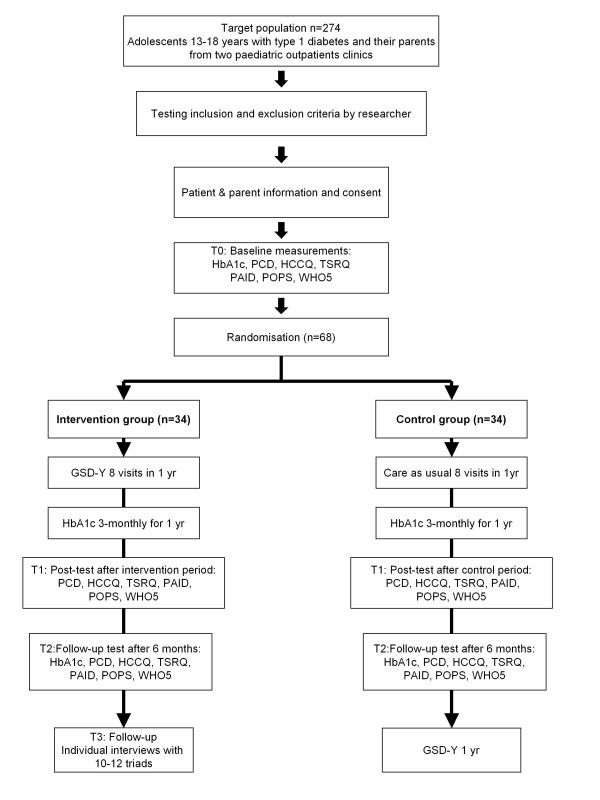
METHODS/DESIGN: Using a mixed methods design comprising a randomised controlled trial and a nested qualitative evaluation, we will recruit 68 adolescents age 13-18 years with type 1 diabetes (HbA1c > 8.0%) and their parents from 2 Danish hospitals and randomise into GSD-Y or control groups. During an 8-12 month period, the GSD-Y group will complete 8 outpatient GSD-Y visits, and the control group will completes an equal number of standard visits. The primary outcome is HbA1c. Secondary outcomes include the following: number of self-monitored blood glucose values and levels of autonomous motivation, involvement and autonomy support from parents, autonomy support from HCPs, perceived competence in managing diabetes, well-being, and diabetes-related problems. Primary and secondary outcomes will be evaluated within and between groups by comparing data from baseline, after completion of the visits, and again after a 6-month follow-up. To illustrate how GSD-Y influences glycaemic control and the development of life skills, 10-12 GSD-Y visits will be recorded during the intervention and analysed qualitatively together with individual interviews carried out after follow-up.
This study will provide evidence of the effectiveness of using a GSD-Y intervention with three parties on HbA1c and life skills and the feasibility of integrating the intervention into routine outpatient clinic visits. Danish Data Association ref nr. 2008-41-2322.
ISRCTN54243636.
由于青少年在心理社会需求和糖尿病管理之间存在优先顺序的冲突,因此 1 型糖尿病青少年面临着艰巨的挑战。这种冲突常常导致血糖控制不佳,以及青少年和家长之间的不和。因此,青少年-家长冲突是医疗保健提供者(HCP)在试图让青少年和家长共同参与改善血糖控制时需要克服的一个障碍。目前缺乏涉及三方(即青少年、家长和 HCP)并整合到常规门诊就诊中的循证干预措施。已证明指导性自我决定方法在成人护理中有效,并已针对青少年和家长进行了调整(青少年指导性自我决定方法(GSD-Y)),用于儿科糖尿病门诊。我们的目标是测试在常规儿科门诊就诊中使用 GSD-Y 是否会降低血红蛋白 A1c(HbA1c)浓度并提高青少年的生活技能,与对照组相比。
方法/设计:使用混合方法设计,包括一项随机对照试验和一项嵌套定性评估,我们将从丹麦的 2 家医院招募 68 名年龄在 13-18 岁之间患有 1 型糖尿病(HbA1c>8.0%)的青少年及其父母,并将其随机分为 GSD-Y 组或对照组。在 8-12 个月的时间里,GSD-Y 组将完成 8 次门诊 GSD-Y 就诊,对照组将完成相同数量的标准就诊。主要结局是 HbA1c。次要结局包括以下内容:自我监测血糖值的数量以及来自父母的自主动机、参与度和自主支持水平,来自 HCP 的自主支持水平,管理糖尿病的能力感,幸福感以及与糖尿病相关的问题。通过比较基线时、就诊结束时和 6 个月随访时的数据,在组内和组间评估主要和次要结局。为了说明 GSD-Y 如何影响血糖控制和生活技能的发展,将在干预期间记录 10-12 次 GSD-Y 就诊,并与随访后进行的个人访谈一起进行定性分析。
这项研究将提供使用三方 GSD-Y 干预措施对 HbA1c 和生活技能的有效性证据,并证明将干预措施整合到常规门诊就诊中的可行性。丹麦数据协会编号 2008-41-2322。
ISRCTN54243636。