Department of Intensive Care Medicine, Bern University Hospital (Inselspital), and University of Bern, Freiburgstrasse, CH-3010 Bern, Switzerland.
Crit Care. 2011 Jun 15;15(3):R148. doi: 10.1186/cc10273.
Acute hemodynamic instability increases morbidity and mortality. We investigated whether early non-invasive cardiac output monitoring enhances hemodynamic stabilization and improves outcome.
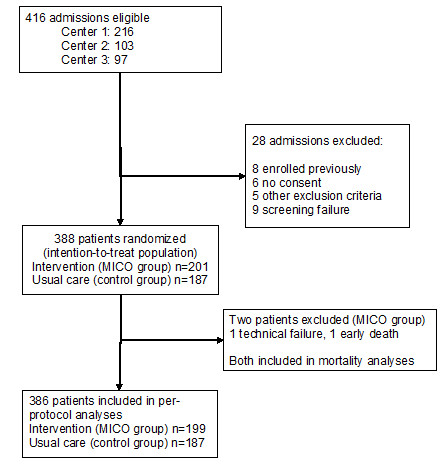
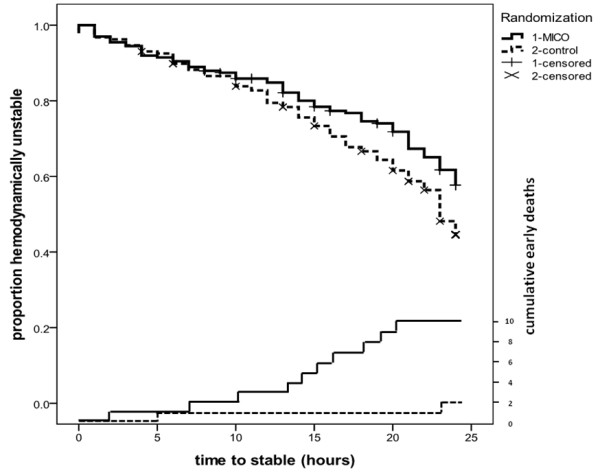
A multicenter, randomized controlled trial was conducted in three European university hospital intensive care units in 2006 and 2007. A total of 388 hemodynamically unstable patients identified during their first six hours in the intensive care unit (ICU) were randomized to receive either non-invasive cardiac output monitoring for 24 hrs (minimally invasive cardiac output/MICO group; n = 201) or usual care (control group; n = 187). The main outcome measure was the proportion of patients achieving hemodynamic stability within six hours of starting the study.
The number of hemodynamic instability criteria at baseline (MICO group mean 2.0 (SD 1.0), control group 1.8 (1.0); P = .06) and severity of illness (SAPS II score; MICO group 48 (18), control group 48 (15); P = .86)) were similar. At 6 hrs, 45 patients (22%) in the MICO group and 52 patients (28%) in the control group were hemodynamically stable (mean difference 5%; 95% confidence interval of the difference -3 to 14%; P = .24). Hemodynamic support with fluids and vasoactive drugs, and pulmonary artery catheter use (MICO group: 19%, control group: 26%; P = .11) were similar in the two groups. The median length of ICU stay was 2.0 (interquartile range 1.2 to 4.6) days in the MICO group and 2.5 (1.1 to 5.0) days in the control group (P = .38). The hospital mortality was 26% in the MICO group and 21% in the control group (P = .34).
Minimally-invasive cardiac output monitoring added to usual care does not facilitate early hemodynamic stabilization in the ICU, nor does it alter the hemodynamic support or outcome. Our results emphasize the need to evaluate technologies used to measure stroke volume and cardiac output--especially their impact on the process of care--before any large-scale outcome studies are attempted.
The study was registered at ClinicalTrials.gov (Clinical Trials identifier NCT00354211).
急性血流动力学不稳定会增加发病率和死亡率。我们研究了早期非侵入性心输出量监测是否能增强血流动力学稳定性并改善预后。
2006 年至 2007 年,在欧洲三所大学附属医院的重症监护病房进行了一项多中心、随机对照试验。在重症监护病房(ICU)的头 6 小时内,共有 388 名血流动力学不稳定的患者被随机分为接受 24 小时非侵入性心输出量监测(微创心输出量/MICO 组;n = 201)或常规护理(对照组;n = 187)。主要观察指标是开始研究后 6 小时内达到血流动力学稳定的患者比例。
基线时血流动力学不稳定标准的数量(MICO 组平均值 2.0(SD 1.0),对照组 1.8(1.0);P =.06)和疾病严重程度(SAPS II 评分;MICO 组 48(18),对照组 48(15);P =.86)相似。6 小时时,MICO 组 45 名(22%)患者和对照组 52 名(28%)患者血流动力学稳定(平均差异 5%;差异 95%置信区间为-3 至 14%;P =.24)。两组之间的液体和血管活性药物的血流动力学支持以及肺动脉导管的使用(MICO 组:19%,对照组:26%;P =.11)相似。MICO 组 ICU 住院时间中位数为 2.0(四分位距 1.2 至 4.6)天,对照组为 2.5(1.1 至 5.0)天(P =.38)。MICO 组的医院死亡率为 26%,对照组为 21%(P =.34)。
微创心输出量监测与常规护理联合使用并不能促进 ICU 早期血流动力学稳定,也不能改变血流动力学支持或预后。我们的结果强调,在尝试任何大规模的结果研究之前,需要评估用于测量心输出量的技术,尤其是其对护理过程的影响。
该研究在 ClinicalTrials.gov 注册(临床试验标识符 NCT00354211)。