Pulmonary and Critical Care Medicine Division, The George Washington University MFA, 2150 Pennsylvania Ave, NW, Washington, DC 20037, USA.
Crit Care. 2011 Jul 12;15(4):R167. doi: 10.1186/cc10309.
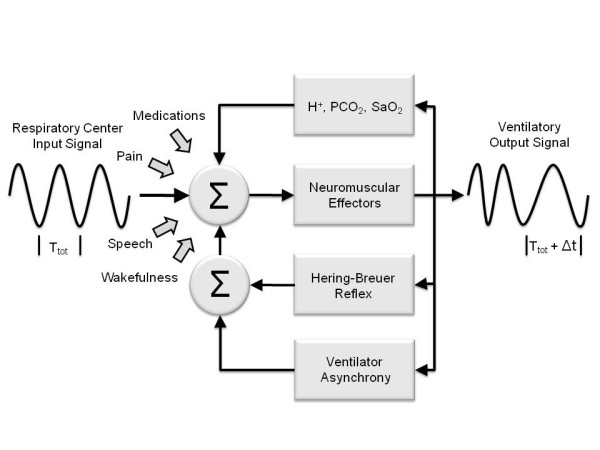
Adequate ventilatory support of critically ill patients depends on prompt recognition of ventilator asynchrony, as asynchrony is associated with worse outcomes.We compared an automatic method of patient-ventilator asynchrony monitoring, based on airway flow frequency analysis, to the asynchrony index (AI) determined visually from airway tracings.
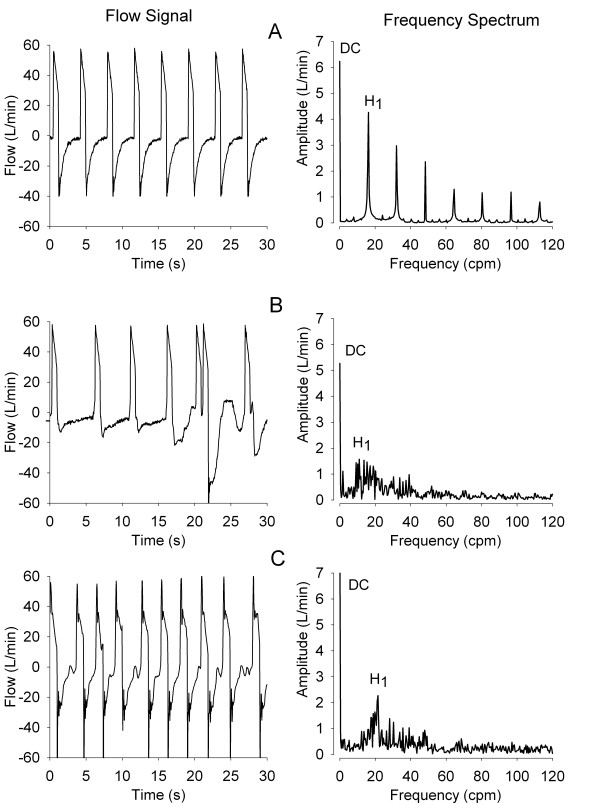
This was a prospective, sequential observational study of 110 mechanically ventilated adults. All eligible ventilated patients were enrolled. No clinical interventions were performed. Airway flow and pressure signals were sampled digitally for two hours. The frequency spectrum of the airway flow signal, processed to include only its expiratory phase, was calculated with the Cooley-Tukey Fast Fourier Transform method at 2.5 minute intervals. The amplitude ratio of the first harmonic peak (H1) to that of zero frequency (DC), or H1/DC, was taken as a measure of spectral organization. AI values were obtained at 30-minute intervals and compared to corresponding measures of H1/DC.
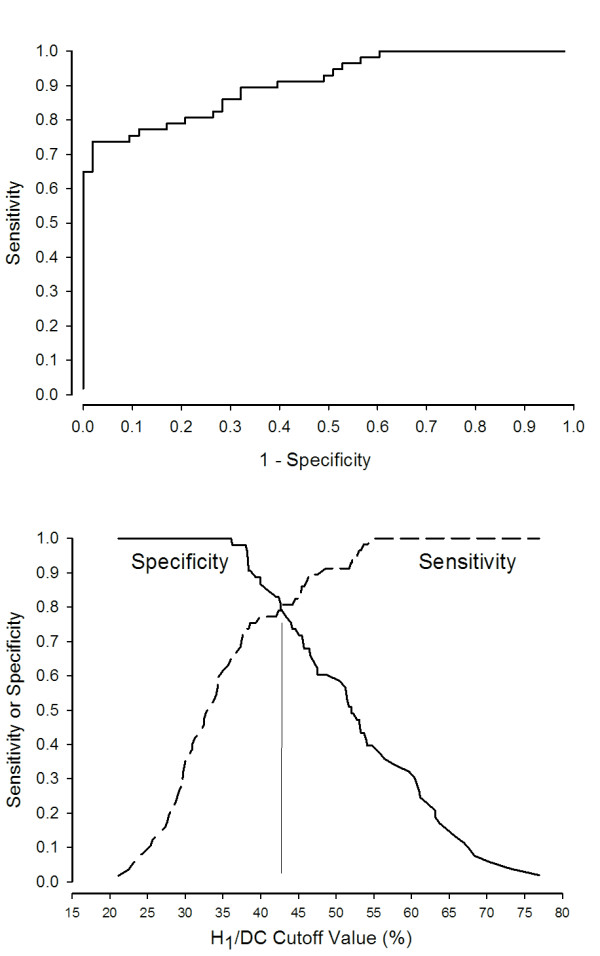
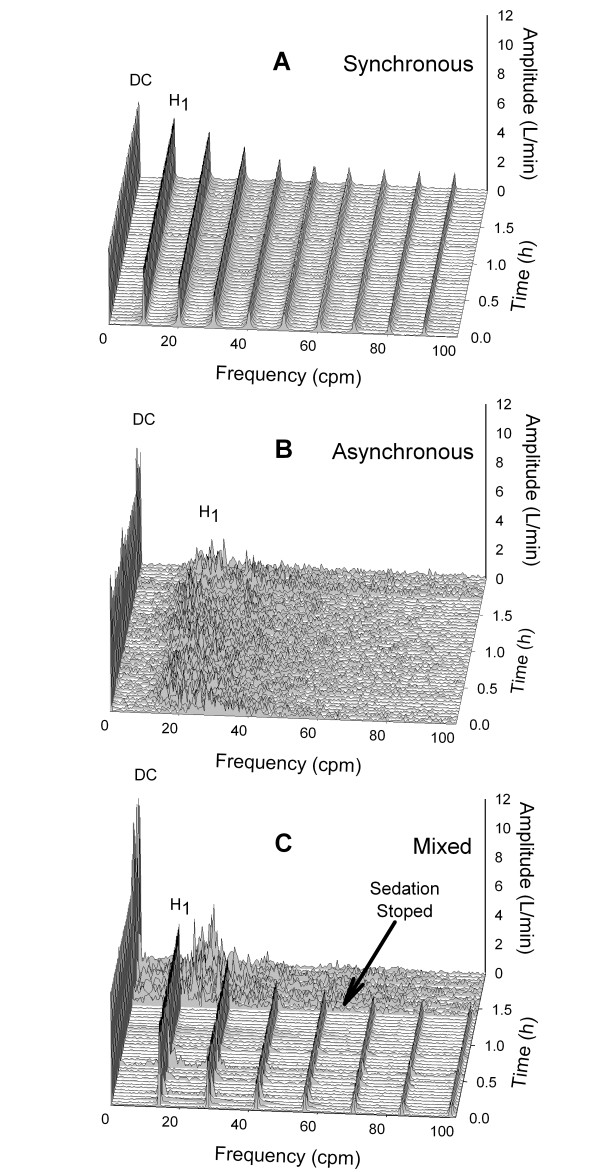
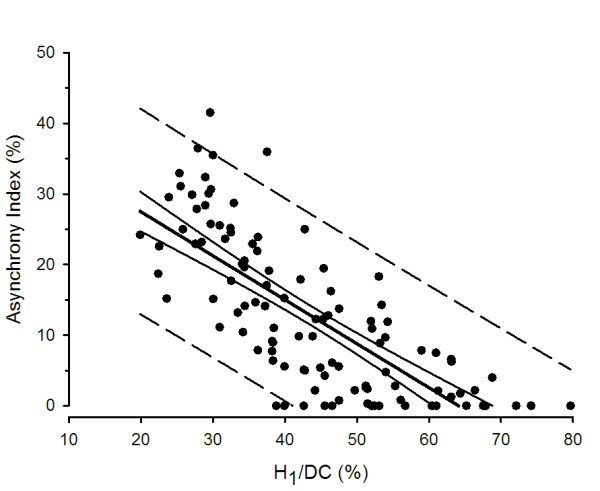
The frequency spectrum of synchronized patients was characterized by sharply defined peaks spaced at multiples of mean respiratory rate. The spectrum of asynchronous patients was less organized, showing lower and wider H1 peaks and disappearance of higher frequency harmonics. H1/DC was inversely related to AI (n = 110; r2 = 0.57; P < 0.0001). Asynchrony, defined by AI > 10%, was associated H1/DC < 43% with 83% sensitivity and specificity.
Spectral analysis of airway flow provides an automatic, non-invasive assessment of ventilator asynchrony at fixed short intervals. This method can be adapted to ventilator systems as a clinical monitor of asynchrony.
危重病患者的充分通气支持取决于对通气机不同步的快速识别,因为不同步与更差的预后相关。我们比较了一种基于气道流量频率分析的自动患者-通气机不同步监测方法与从气道描记图中确定的不同步指数(AI)。
这是一项对 110 例机械通气成人的前瞻性、连续观察性研究。所有符合条件的通气患者均被纳入研究。未进行任何临床干预。气道流量和压力信号以数字方式每 2 小时采集一次。通过科利-图基快速傅里叶变换方法对气道流量信号的频谱进行计算,该方法仅包括其呼气相,以 2.5 分钟的间隔进行。将第一谐波峰值(H1)与零频率(DC)的幅度比(H1/DC)作为频谱组织的度量。每隔 30 分钟获取 AI 值,并将其与相应的 H1/DC 进行比较。
同步患者的频谱特征是具有明确间隔的锐定义峰值,间隔为平均呼吸频率的倍数。不同步患者的频谱组织性较差,显示出较低且较宽的 H1 峰值,并且较高频率的谐波消失。H1/DC 与 AI 呈负相关(n = 110;r2 = 0.57;P < 0.0001)。AI > 10%定义的不同步与 H1/DC < 43%具有 83%的灵敏度和特异性相关。
气道流量的频谱分析可在固定的短间隔内自动、无创地评估通气机不同步。这种方法可以作为通气机不同步的临床监测器,适用于各种通气系统。