Division of Medical Microbiology and Institute for Infectious Diseases and Molecular Medicine, University of Cape Town, Cape Town, South Africa.
Lancet Infect Dis. 2011 Nov;11(11):819-24. doi: 10.1016/S1473-3099(11)70167-0. Epub 2011 Jul 19.
WHO recommends that Xpert MTB/RIF replaces smear microscopy for initial diagnosis of suspected HIV-associated tuberculosis or multidrug-resistant pulmonary tuberculosis, but no data exist for its use in children. We aimed to assess the accuracy of the test for the diagnosis of pulmonary tuberculosis in children in an area with high tuberculosis and HIV prevalences.
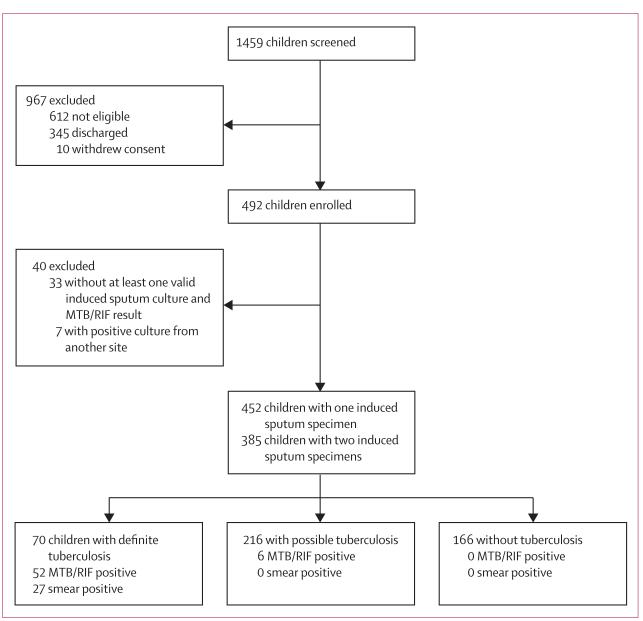
In this prospective, descriptive study, we enrolled children aged 15 years or younger who had been admitted to one of two hospitals in Cape Town, South Africa, with suspected pulmonary tuberculosis between Feb 19, 2009, and Nov 30, 2010. We compared the diagnostic accuracy of MTB/RIF and concentrated, fluorescent acid-fast smear with a reference standard of liquid culture from two sequential induced sputum specimens (primary analysis).
452 children (median age 19·4 months, IQR 11·1-46·2) had at least one induced sputum specimen; 108 children (24%) had HIV infection. 27 children (6%) had a positive smear result, 70 (16%) had a positive culture result, and 58 (13%) had a positive MTB/RIF test result. With mycobacterial culture as the reference standard, MTB/RIF tests when done on two induced sputum samples detected twice as many cases (75·9%, 95% CI 64·5-87·2) as did smear microscopy (37·9%, 25·1-50·8), detecting all of 22 smear-positive cases and 22 of 36 (61·1%, 44·4-77·8) smear-negative cases. For smear-negative cases, the incremental increase in sensitivity from testing a second specimen was 27·8% for MTB/RIF, compared with 13·8% for culture. The specificity of MTB/RIF was 98·8% (97·6-99·9). MTB/RIF results were available in median 1 day (IQR 0-4) compared with median 12 days (9-17) for culture (p<0·0001).
MTB/RIF testing of two induced sputum specimens is warranted as the first-line diagnostic test for children with suspected pulmonary tuberculosis.
National Institutes of Health, the National Health Laboratory Service Research Trust, the Medical Research Council of South Africa, and Wellcome Trust.
世界卫生组织建议使用 Xpert MTB/RIF 取代涂片显微镜检查,作为初始诊断疑似 HIV 相关结核病或耐多药肺结核的方法,但目前尚无其在儿童中的使用数据。我们旨在评估该检测方法在高结核和 HIV 流行地区用于诊断儿童肺结核的准确性。
在这项前瞻性描述性研究中,我们纳入了 2009 年 2 月 19 日至 2010 年 11 月 30 日期间在南非开普敦的两家医院因疑似肺结核而入院的 15 岁以下儿童。我们将 MTB/RIF 和浓缩、荧光抗酸染色的诊断准确性与两份连续诱导痰标本的液体培养的参考标准进行了比较(主要分析)。
452 名儿童(中位年龄 19.4 个月,IQR 11.1-46.2)至少有一份诱导痰标本;108 名儿童(24%)感染了 HIV。27 名儿童(6%)的涂片结果阳性,70 名儿童(16%)的培养结果阳性,58 名儿童(13%)的 MTB/RIF 检测结果阳性。以分枝杆菌培养为参考标准,两次诱导痰样本的 MTB/RIF 检测可检测出两倍的病例(75.9%,95%CI 64.5-87.2),而涂片显微镜检查的检测率为 37.9%(25.1-50.8),可检测到所有 22 例涂片阳性病例和 36 例(61.1%,44.4-77.8)涂片阴性病例。对于涂片阴性病例,MTB/RIF 检测第二次标本的敏感性增加了 27.8%,而培养的敏感性增加了 13.8%。MTB/RIF 的特异性为 98.8%(97.6-99.9)。MTB/RIF 结果的中位获得时间为 1 天(IQR 0-4),而培养的中位获得时间为 12 天(9-17)(p<0.0001)。
对于疑似肺结核的儿童,建议使用两次诱导痰样本的 MTB/RIF 检测作为一线诊断检测方法。
美国国立卫生研究院、国家卫生实验室服务研究信托基金、南非医学研究理事会和惠康信托基金会。