Kay Alexander W, González Fernández Lucia, Takwoingi Yemisi, Eisenhut Michael, Detjen Anne K, Steingart Karen R, Mandalakas Anna M
The Global Tuberculosis Program, Texas Children's Hospital, Section of Global and Immigrant Health, Department of Pediatrics, Baylor College of Medicine, Houston, Texas, USA.
Department of Paediatrics, Baylor College of Medicine, Houston, Texas, USA.
Cochrane Database Syst Rev. 2020 Aug 27;8(8):CD013359. doi: 10.1002/14651858.CD013359.pub2.
Every year, at least one million children become ill with tuberculosis and around 200,000 children die. Xpert MTB/RIF and Xpert Ultra are World Health Organization (WHO)-recommended rapid molecular tests that simultaneously detect tuberculosis and rifampicin resistance in adults and children with signs and symptoms of tuberculosis, at lower health system levels. To inform updated WHO guidelines on molecular assays, we performed a systematic review on the diagnostic accuracy of these tests in children presumed to have active tuberculosis.
Primary objectives • To determine the diagnostic accuracy of Xpert MTB/RIF and Xpert Ultra for (a) pulmonary tuberculosis in children presumed to have tuberculosis; (b) tuberculous meningitis in children presumed to have tuberculosis; (c) lymph node tuberculosis in children presumed to have tuberculosis; and (d) rifampicin resistance in children presumed to have tuberculosis - For tuberculosis detection, index tests were used as the initial test, replacing standard practice (i.e. smear microscopy or culture) - For detection of rifampicin resistance, index tests replaced culture-based drug susceptibility testing as the initial test Secondary objectives • To compare the accuracy of Xpert MTB/RIF and Xpert Ultra for each of the four target conditions • To investigate potential sources of heterogeneity in accuracy estimates - For tuberculosis detection, we considered age, disease severity, smear-test status, HIV status, clinical setting, specimen type, high tuberculosis burden, and high tuberculosis/HIV burden - For detection of rifampicin resistance, we considered multi-drug-resistant tuberculosis burden • To compare multiple Xpert MTB/RIF or Xpert Ultra results (repeated testing) with the initial Xpert MTB/RIF or Xpert Ultra result SEARCH METHODS: We searched the Cochrane Infectious Diseases Group Specialized Register, MEDLINE, Embase, Science Citation Index, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Scopus, the WHO International Clinical Trials Registry Platform, ClinicalTrials.gov, and the International Standard Randomized Controlled Trials Number (ISRCTN) Registry up to 29 April 2019, without language restrictions.
Randomized trials, cross-sectional trials, and cohort studies evaluating Xpert MTB/RIF or Xpert Ultra in HIV-positive and HIV-negative children younger than 15 years. Reference standards comprised culture or a composite reference standard for tuberculosis and drug susceptibility testing or MTBDRplus (molecular assay for detection of Mycobacterium tuberculosis and drug resistance) for rifampicin resistance. We included studies evaluating sputum, gastric aspirate, stool, nasopharyngeal or bronchial lavage specimens (pulmonary tuberculosis), cerebrospinal fluid (tuberculous meningitis), fine needle aspirates, or surgical biopsy tissue (lymph node tuberculosis).
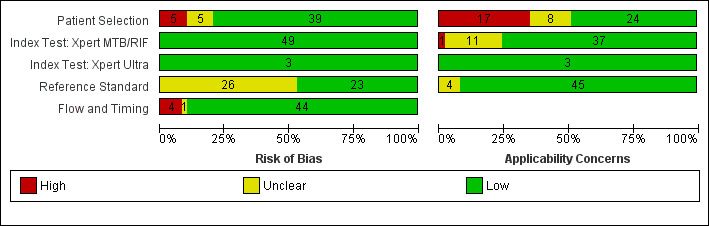
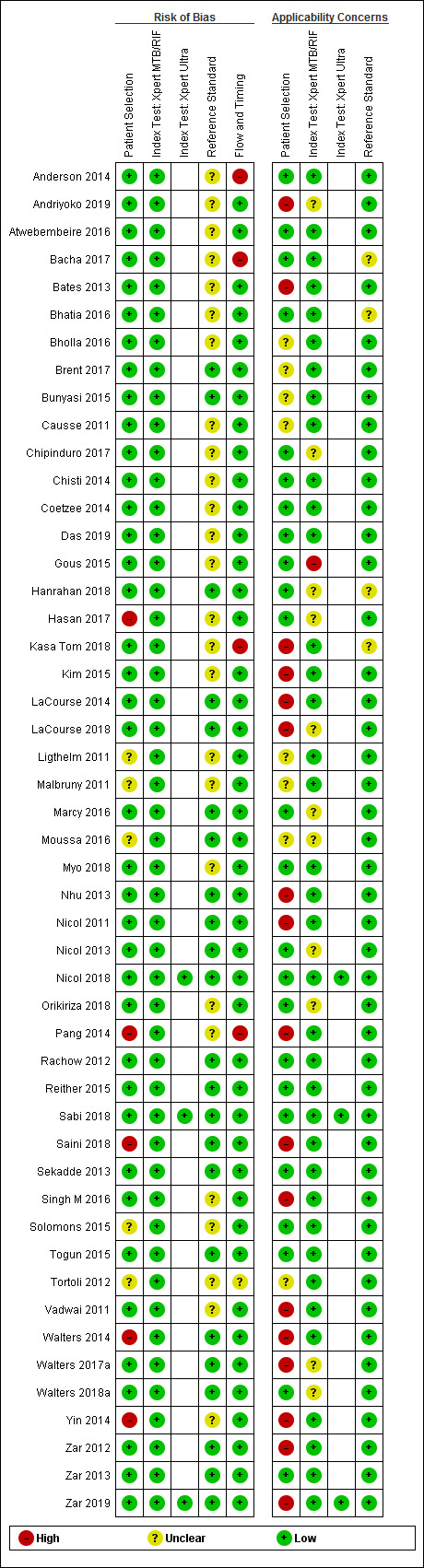
Two review authors independently extracted data and assessed study quality using the Quality Assessment of Studies of Diagnostic Accuracy - Revised (QUADAS-2). For each target condition, we used the bivariate model to estimate pooled sensitivity and specificity with 95% confidence intervals (CIs). We stratified all analyses by type of reference standard. We assessed certainty of evidence using the GRADE approach.
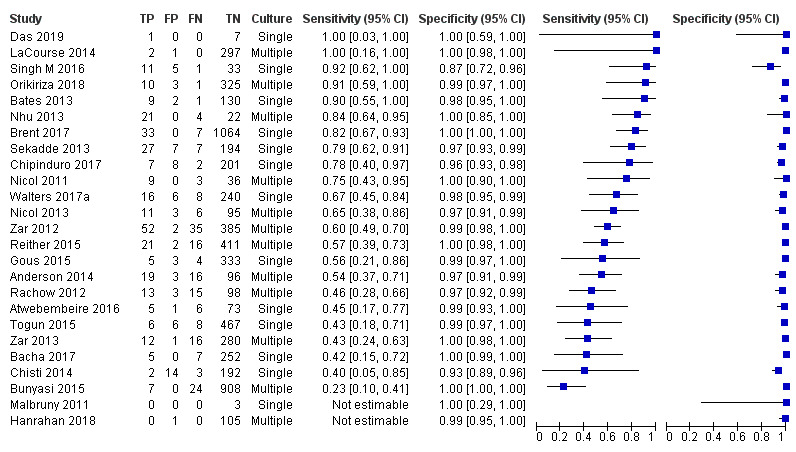
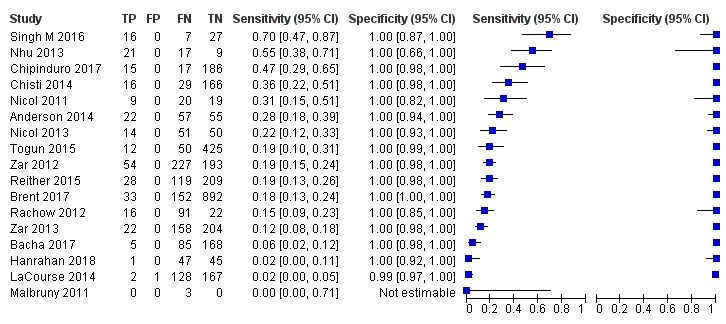
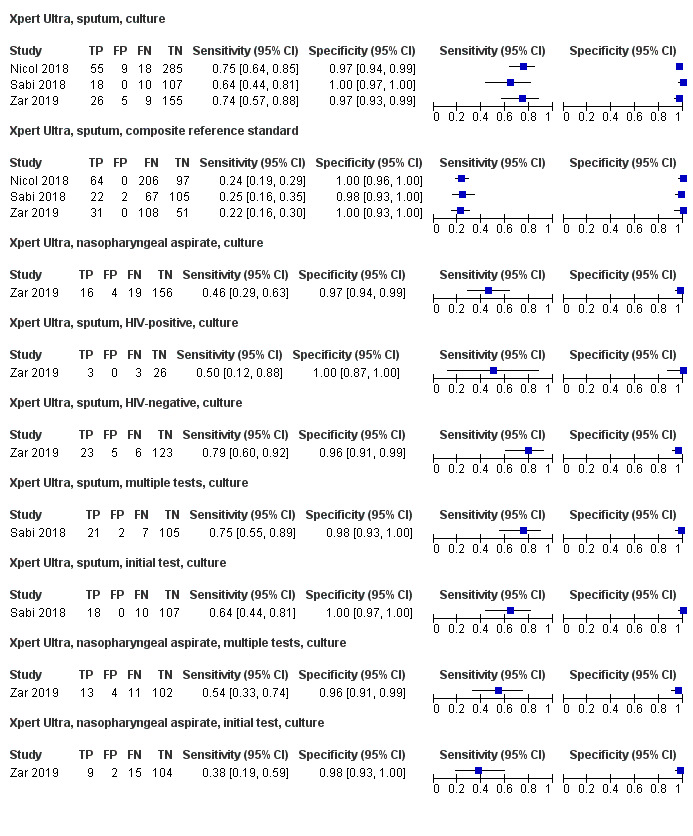
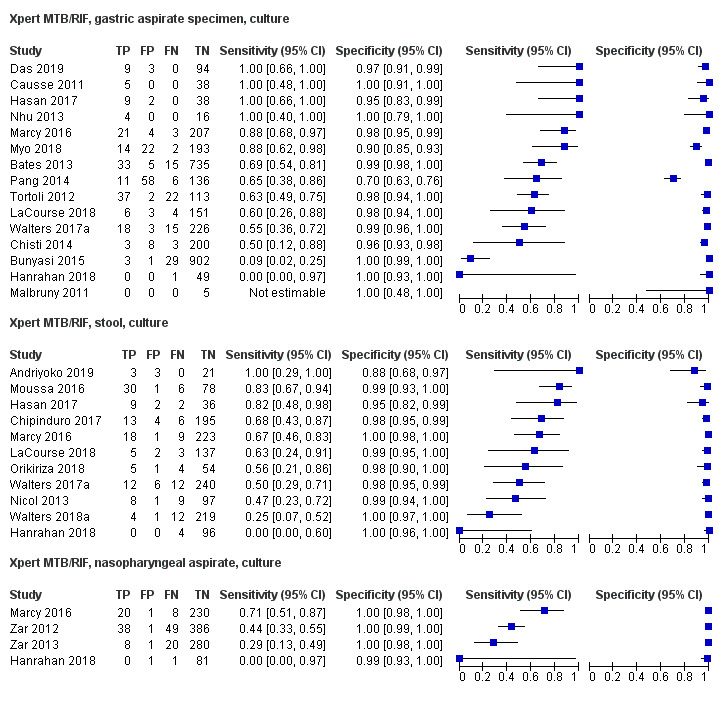
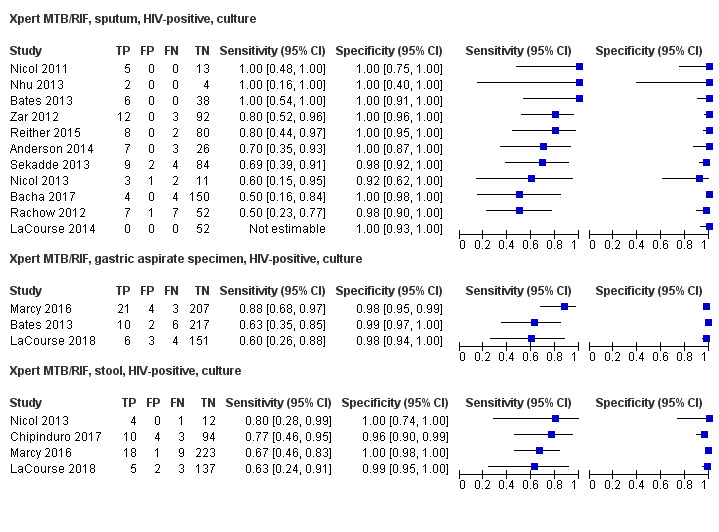
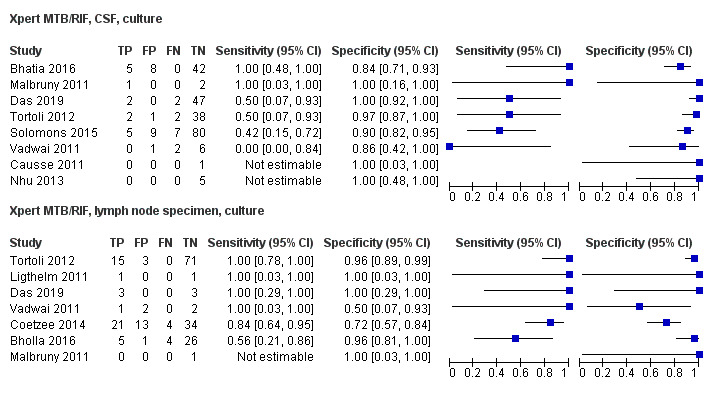
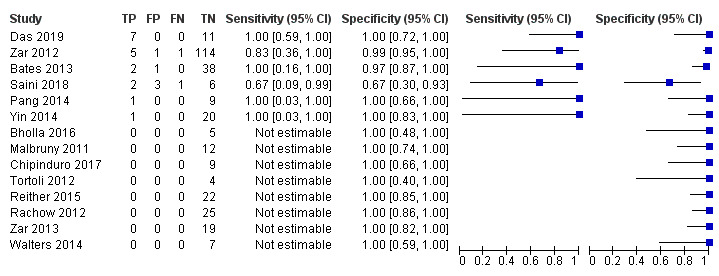
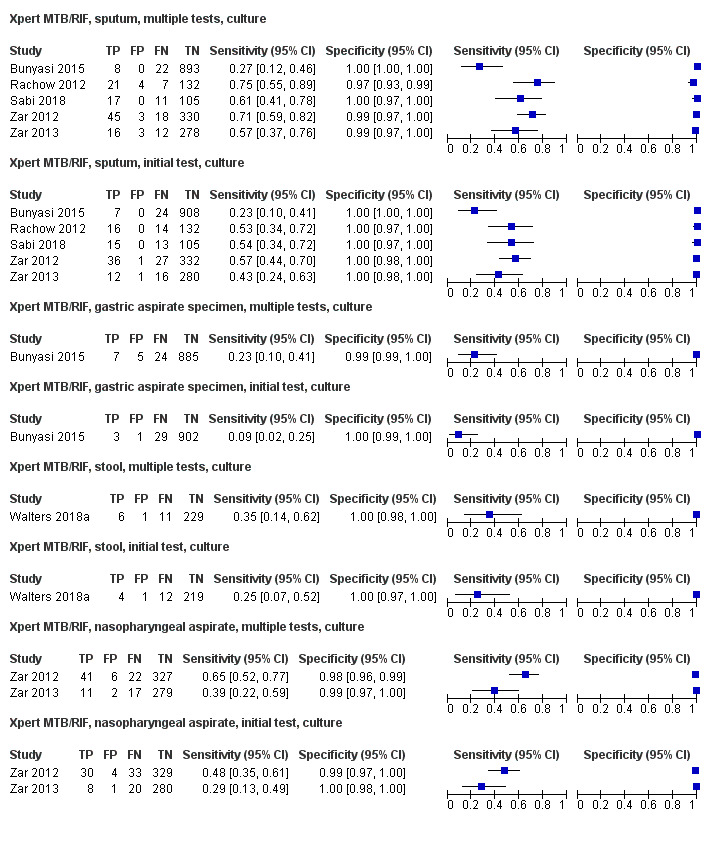
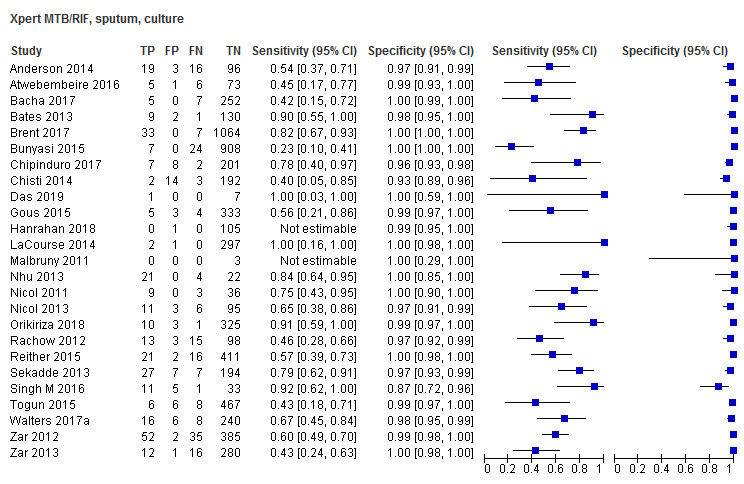
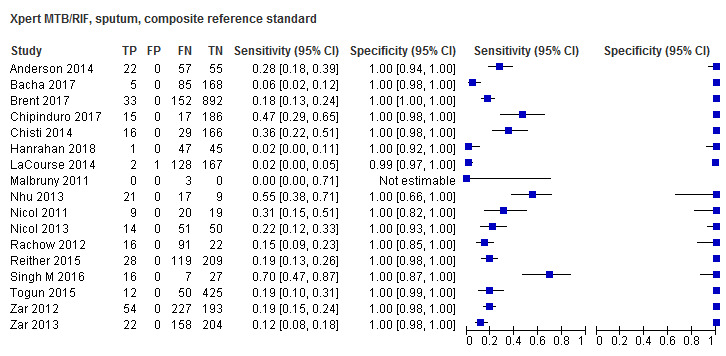
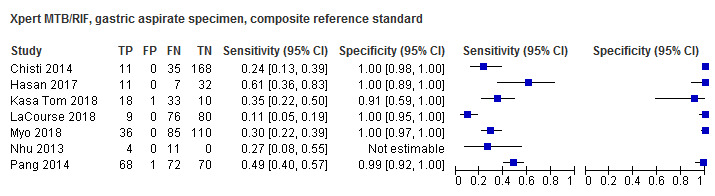
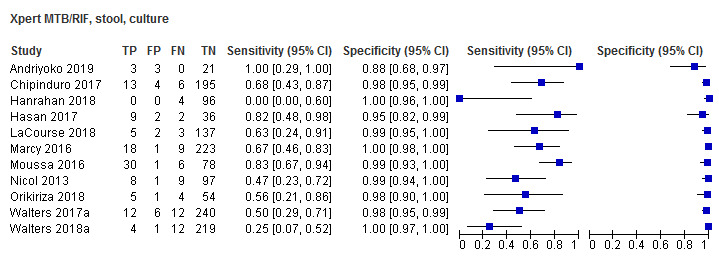
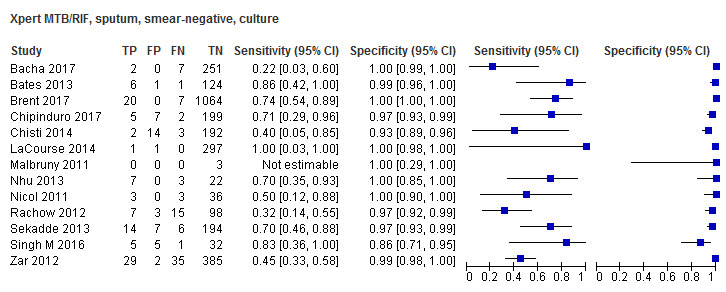
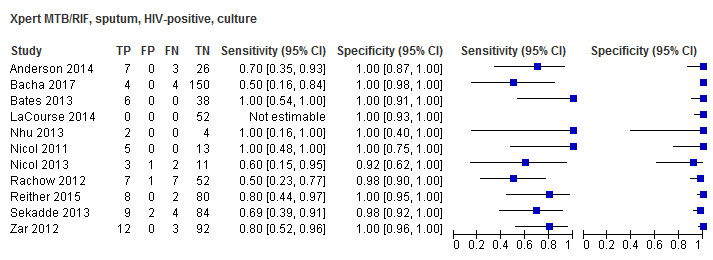
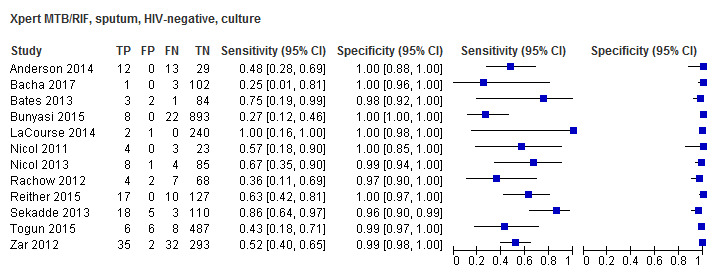
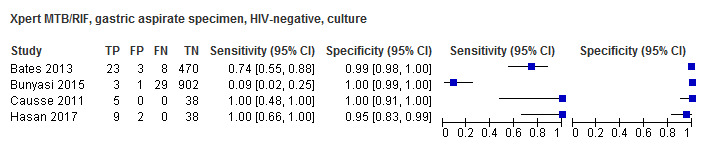
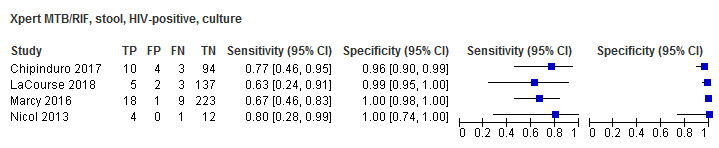
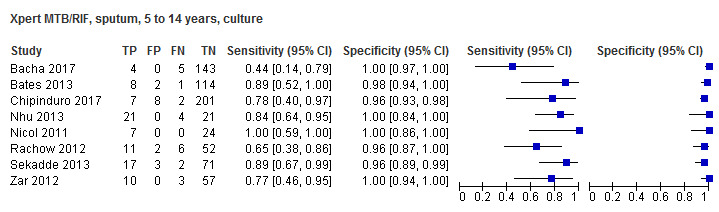
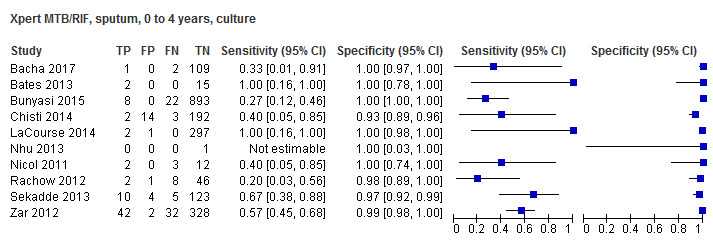
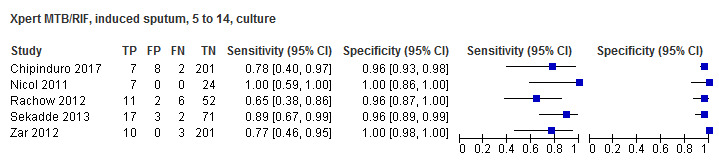
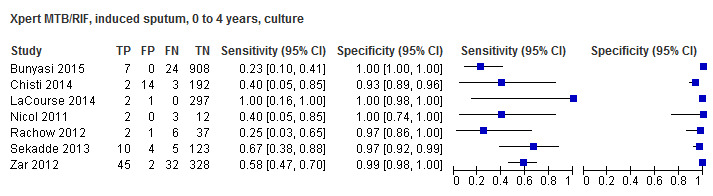
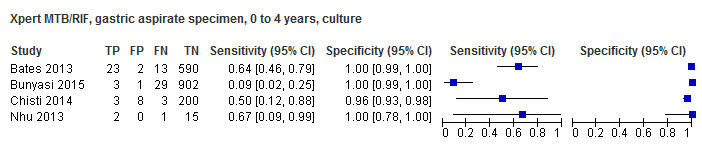
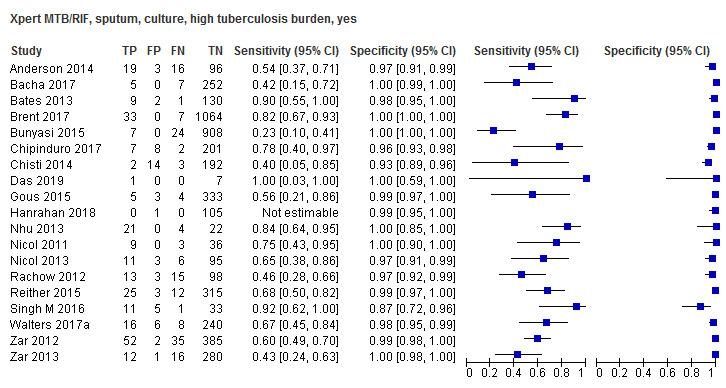
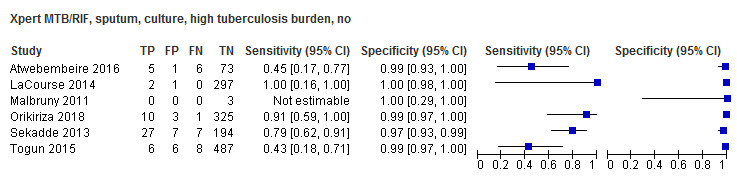
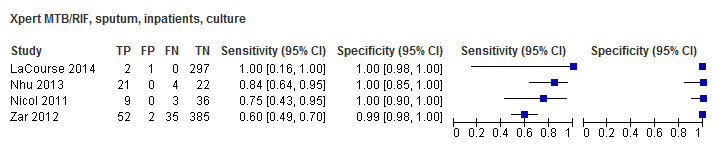
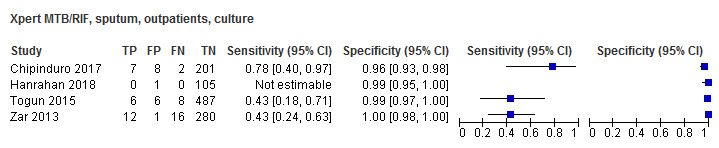
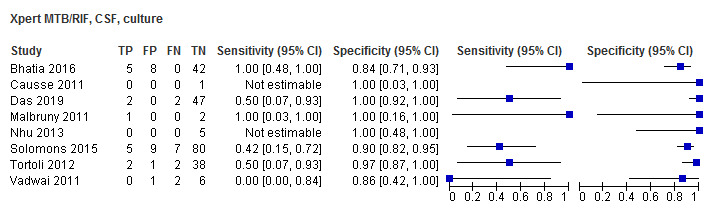
For pulmonary tuberculosis, 299 data sets (68,544 participants) were available for analysis; for tuberculous meningitis, 10 data sets (423 participants) were available; for lymph node tuberculosis, 10 data sets (318 participants) were available; and for rifampicin resistance, 14 data sets (326 participants) were available. Thirty-nine studies (80%) took place in countries with high tuberculosis burden. Risk of bias was low except for the reference standard domain, for which risk of bias was unclear because many studies collected only one specimen for culture. Detection of pulmonary tuberculosis For sputum specimens, Xpert MTB/RIF pooled sensitivity (95% CI) and specificity (95% CI) verified by culture were 64.6% (55.3% to 72.9%) (23 studies, 493 participants; moderate-certainty evidence) and 99.0% (98.1% to 99.5%) (23 studies, 6119 participants; moderate-certainty evidence). For other specimen types (nasopharyngeal aspirate, 4 studies; gastric aspirate, 14 studies; stool, 11 studies), Xpert MTB/RIF pooled sensitivity ranged between 45.7% and 73.0%, and pooled specificity ranged between 98.1% and 99.6%. For sputum specimens, Xpert Ultra pooled sensitivity (95% CI) and specificity (95% CI) verified by culture were 72.8% (64.7% to 79.6%) (3 studies, 136 participants; low-certainty evidence) and 97.5% (95.8% to 98.5%) (3 studies, 551 participants; high-certainty evidence). For nasopharyngeal specimens, Xpert Ultra sensitivity (95% CI) and specificity (95% CI) were 45.7% (28.9% to 63.3%) and 97.5% (93.7% to 99.3%) (1 study, 195 participants). For all specimen types, Xpert MTB/RIF and Xpert Ultra sensitivity were lower against a composite reference standard than against culture. Detection of tuberculous meningitis For cerebrospinal fluid, Xpert MTB/RIF pooled sensitivity and specificity, verified by culture, were 54.0% (95% CI 27.8% to 78.2%) (6 studies, 28 participants; very low-certainty evidence) and 93.8% (95% CI 84.5% to 97.6%) (6 studies, 213 participants; low-certainty evidence). Detection of lymph node tuberculosis For lymph node aspirates or biopsies, Xpert MTB/RIF pooled sensitivity and specificity, verified by culture, were 90.4% (95% CI 55.7% to 98.6%) (6 studies, 68 participants; very low-certainty evidence) and 89.8% (95% CI 71.5% to 96.8%) (6 studies, 142 participants; low-certainty evidence). Detection of rifampicin resistance Xpert MTB/RIF pooled sensitivity and specificity were 90.0% (67.6% to 97.5%) (6 studies, 20 participants; low-certainty evidence) and 98.3% (87.7% to 99.8%) (6 studies, 203 participants; moderate-certainty evidence).
AUTHORS' CONCLUSIONS: We found Xpert MTB/RIF sensitivity to vary by specimen type, with gastric aspirate specimens having the highest sensitivity followed by sputum and stool, and nasopharyngeal specimens the lowest; specificity in all specimens was > 98%. Compared with Xpert MTB/RIF, Xpert Ultra sensitivity in sputum was higher and specificity slightly lower. Xpert MTB/RIF was accurate for detection of rifampicin resistance. Xpert MTB/RIF was sensitive for diagnosing lymph node tuberculosis. For children with presumed tuberculous meningitis, treatment decisions should be based on the entirety of clinical information and treatment should not be withheld based solely on an Xpert MTB/RIF result. The small numbers of studies and participants, particularly for Xpert Ultra, limits our confidence in the precision of these estimates.
每年至少有100万儿童患结核病,约20万儿童死亡。Xpert MTB/RIF和Xpert Ultra是世界卫生组织(WHO)推荐的快速分子检测方法,可在较低层级的卫生系统中同时检测有结核病体征和症状的成人及儿童的结核病和利福平耐药性。为了为WHO关于分子检测方法的更新指南提供依据,我们对这些检测方法在疑似患有活动性结核病儿童中的诊断准确性进行了系统评价。
主要目的 • 确定Xpert MTB/RIF和Xpert Ultra对于以下情况的诊断准确性:(a)疑似患有结核病儿童的肺结核;(b)疑似患有结核病儿童的结核性脑膜炎;(c)疑似患有结核病儿童的淋巴结结核;(d)疑似患有结核病儿童的利福平耐药性 - 对于结核病检测,将索引检测用作初始检测,取代标准做法(即涂片显微镜检查或培养) - 对于利福平耐药性检测,索引检测取代基于培养的药物敏感性检测作为初始检测 次要目的 • 比较Xpert MTB/RIF和Xpert Ultra在四种目标情况下各自的准确性 • 调查准确性估计中潜在的异质性来源 - 对于结核病检测,我们考虑了年龄、疾病严重程度、涂片检测状态、HIV状态、临床环境、标本类型、高结核病负担和高结核病/HIV负担 - 对于利福平耐药性检测,我们考虑了耐多药结核病负担 • 比较多个Xpert MTB/RIF或Xpert Ultra结果(重复检测)与初始Xpert MTB/RIF或Xpert Ultra结果 检索方法:我们检索了Cochrane传染病小组专业注册库、MEDLINE、Embase、科学引文索引、护理学与健康相关文献累积索引(CINAHL)、Scopus、WHO国际临床试验注册平台、ClinicalTrials.gov以及国际标准随机对照试验编号(ISRCTN)注册库,检索截至2019年4月29日,无语言限制。
评估Xpert MTB/RIF或Xpert Ultra在15岁以下HIV阳性和HIV阴性儿童中的随机试验、横断面试验和队列研究。参考标准包括培养或结核病的综合参考标准以及利福平耐药性的药物敏感性检测或MTBDRplus(检测结核分枝杆菌和耐药性的分子检测方法)。我们纳入了评估痰液、胃液抽吸物、粪便、鼻咽或支气管灌洗标本(肺结核)、脑脊液(结核性脑膜炎)、细针抽吸物或手术活检组织(淋巴结结核)的研究。
两位综述作者独立提取数据,并使用诊断准确性研究质量评估 - 修订版(QUADAS - 2)评估研究质量。对于每种目标情况,我们使用双变量模型估计合并敏感性和特异性以及95%置信区间(CI)。我们按参考标准类型对所有分析进行分层。我们使用GRADE方法评估证据的确定性。
对于肺结核,有299个数据集(68,544名参与者)可用于分析;对于结核性脑膜炎,有10个数据集(423名参与者)可用于分析;对于淋巴结结核,有10个数据集(318名参与者)可用于分析;对于利福平耐药性,有14个数据集(326名参与者)可用于分析。39项研究(80%)在结核病负担高的国家进行。除参考标准领域外,偏倚风险较低,该领域偏倚风险不明确,因为许多研究仅收集一份标本用于培养。肺结核检测 对于痰液标本,经培养验证的Xpert MTB/RIF合并敏感性(95%CI)和特异性(95%CI)分别为64.6%(55.3%至72.9%)(23项研究,493名参与者;中等确定性证据)和99.0%(98.1%至99.5%)(23项研究,6119名参与者;中等确定性证据)。对于其他标本类型(鼻咽抽吸物,4项研究;胃液抽吸物, 14项研究;粪便,11项研究),Xpert MTB/RIF合并敏感性在45.7%至73.0%之间,合并特异性在98.1%至99.6%之间。对于痰液标本,经培养验证的Xpert Ultra合并敏感性(95%CI)和特异性(95%CI)分别为72.8%(64.7%至79.6%)(3项研究,136名参与者;低确定性证据)和97.5%(95.8%至9