Cardiology Division, Cardiovascular Center of National Health Insurance Corporation Ilsan Hospital, Goyang, Korea.
Yonsei Med J. 2011 Sep;52(5):717-26. doi: 10.3349/ymj.2011.52.5.717.
It is unknown whether cilostazol pretreatment reduces postprocedural myonecrosis (PPMN). Cilostazol pretreatment reduces PPMN after percutaneous coronary intervention (PCI).
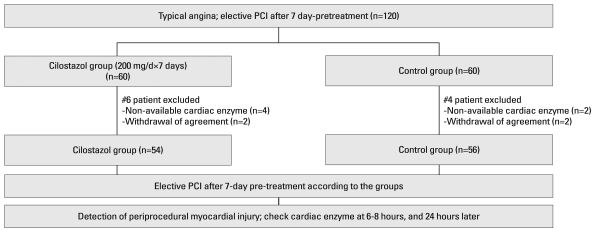
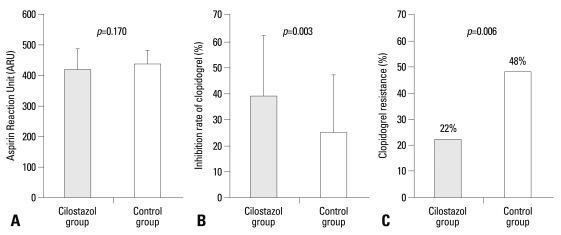
A total of 120 patients with stable angina scheduled for elective PCI were randomly assigned to a 7-day pretreatment with Cilostazol (200 mg/day) or to a control group. Creatine kinase-MB (CK-MB) and cardiac troponin I (cTnI) levels were measured at baseline and at 6 and 24 hours after PCI. The primary end-point was the occurrence of PPMN, defined as any CK-MB elevation above the upper normal limit (UNL). Aspirin and clopidogrel were co-administered for 7 days before PCI, and resistance to these agents was then assayed using the VerifyNow System.
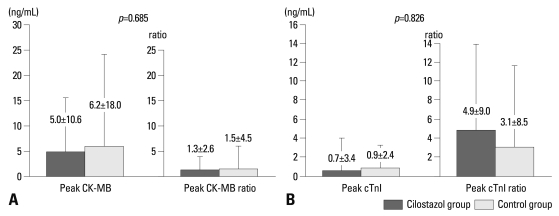
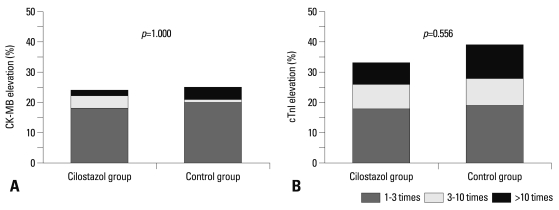
There was no difference in baseline characteristics between the final analyzable cilostazol (n=54) and the control group (n=56). Despite a significantly greater % inhibition of clopidogrel in the cilostazol group (39±23% versus 25±22%, p=0.003), the incidence of PPMN was similar between the cilostazol group (24%) and the control group (25%, p=1.000). The rate of CK-MB elevation at ≥3 times UNL was also similar between the two groups (6% versus 5%, p=0.583). The incidence of cTnI increase over the UNL or to 3 times the UNL was not different between the two groups. There was no significant difference in terms of the rate of adverse events during follow- up, although the cilostazol group showed a tendency to have a slightly higher incidence of entry site hematoma.
This trial demonstrated that adjunctive cilostazol pretreatment might not significantly reduce PPMN after elective PCI in patients with stable angina.
目前尚不清楚西洛他唑预处理是否会减少经皮冠状动脉介入治疗(PCI)后的心肌坏死(PPMN)。西洛他唑预处理可减少 PCI 后的 PPMN。
共 120 例稳定型心绞痛患者拟行选择性 PCI,随机分为西洛他唑(200mg/天)预处理组和对照组。在基线和 PCI 后 6 小时和 24 小时测量肌酸激酶同工酶-MB(CK-MB)和心肌肌钙蛋白 I(cTnI)水平。主要终点是 PPMN 的发生,定义为 CK-MB 升高超过正常上限(UNL)。在 PCI 前 7 天同时给予阿司匹林和氯吡格雷,并使用 VerifyNow 系统检测这些药物的抵抗性。
最终分析的西洛他唑组(n=54)和对照组(n=56)的基线特征无差异。尽管西洛他唑组氯吡格雷的抑制率显著更高(39±23%比 25±22%,p=0.003),但西洛他唑组(24%)和对照组(25%)的 PPMN 发生率相似(p=1.000)。两组 CK-MB 升高至≥3 倍 UNL 的发生率也相似(6%比 5%,p=0.583)。两组 cTnI 升高超过 UNL 或升高至 3 倍 UNL 的发生率无差异。在随访期间,不良事件的发生率没有显著差异,尽管西洛他唑组的穿刺部位血肿发生率略高。
本试验表明,在稳定型心绞痛患者中,选择性 PCI 前辅助西洛他唑预处理可能不会显著减少 PPMN。