Department of Medicine, Cardiology division. Universidade Federal de São Paulo - Escola Paulista de Medicina, São Paulo, SP, Brazil.
Clinics (Sao Paulo). 2011;66(5):889-93. doi: 10.1590/s1807-59322011000500028.
This study aimed to investigate whether previous exercise training could prevent or attenuate acute cardiac alterations after myocardial infarction.
Female rats were submitted to swim training (1 h/day; 5 days/week) or allowed to remain sedentary for 8 weeks. Afterwards, they were randomly assigned to left coronary artery occlusion or sham surgery. After this procedure, the rats remained sedentary for one week until euthanasia. Cardiac structural and functional analyses were performed using Doppler echocardiography. The rats that had a moderate or large infarct size were included in the evaluations. The data (mean ± SEM) were analyzed using a two-way ANOVA model followed by Tukey's post-hoc test.
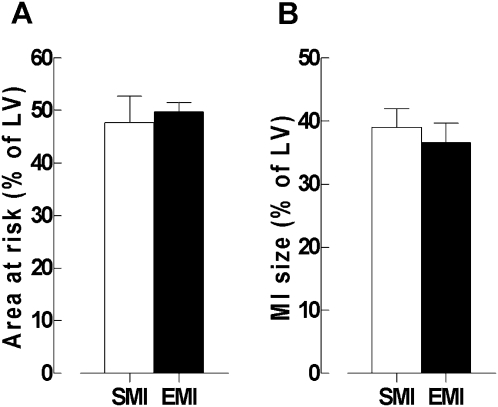
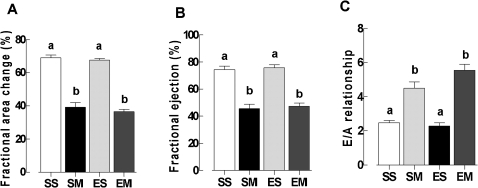
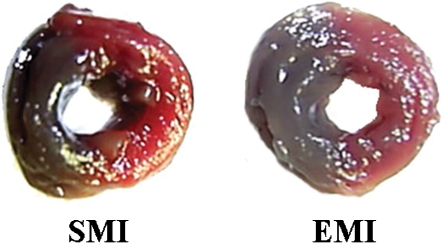
After the surgery, no significant difference between the exercise and sedentary groups was observed in the left ventricular infarct sizes (34.58 ± 3.04 vs. 37.59 ± 3.07). In another group of rats evaluated with Evans blue 1 h after myocardial infarction, no siginificant difference in the area at risk was observed between the exercised and sedentary rats (49.73 ± 1.52 vs. 45.48 ± 3.49). The changes in the left ventricular fractional areas for the exercised and sedentary myocardial infarction groups (36 ± 2% and 39 ± 3%, respectively) were smaller than those for the exercise sham surgery (ES, 67 ± 1%) and sedentary sham surgery (SS, 69 ± 2%) groups. The E/A was higher in the sedentary myocardial infarction (4.4 ± 0.3) and exercised myocardial infarction (5.5 ± 0.3) rats than in the SS (2.4 ± 0.1) and ES (2.2 ± 0.1) rats.
Previous swim training of female rats does not attenuate systolic and diastolic function alterations after myocardial infarction induced by left coronary artery occlusion, suggesting that cardioprotection cannot be provided by exercise training in this experimental model.
本研究旨在探讨先前的运动训练是否可以预防或减轻心肌梗死后的急性心脏改变。
雌性大鼠进行游泳训练(1 小时/天;每周 5 天)或保持 8 周的安静状态。之后,它们被随机分配到左冠状动脉结扎或假手术组。手术后,大鼠保持安静状态 1 周,直到安乐死。使用多普勒超声心动图进行心脏结构和功能分析。将梗死面积中等或较大的大鼠纳入评估。使用双因素方差分析模型(ANOVA)和 Tukey 事后检验对数据(平均值±SEM)进行分析。
手术后,运动组和安静组的左心室梗死面积(34.58 ± 3.04 比 37.59 ± 3.07)之间无显著差异。在另一组大鼠中,在心肌梗死后 1 小时用 Evans 蓝进行评估时,运动和安静大鼠的危险区面积无显著差异(49.73 ± 1.52 比 45.48 ± 3.49)。与运动假手术(ES)和安静假手术(SS)组相比,运动性和安静性心肌梗死组的左心室分数区域变化(分别为 36 ± 2%和 39 ± 3%)较小。在安静性心肌梗死(4.4 ± 0.3)和运动性心肌梗死(5.5 ± 0.3)大鼠中,E/A 比值高于 SS(2.4 ± 0.1)和 ES(2.2 ± 0.1)大鼠。
先前对雌性大鼠进行的游泳训练并不能减轻左冠状动脉结扎引起的心肌梗死后的收缩和舒张功能改变,提示在这种实验模型中,运动训练不能提供心脏保护。