Sonderegger Juerg, Grob Karl R, Kuster Markus S
Department of Hand-, Plastic-, and Reconstructive Surgery, Kantonsspital, St. Gallen, Switzerland;
Orthop Rev (Pavia). 2010 Mar 20;2(1):e4. doi: 10.4081/or.2010.e4.
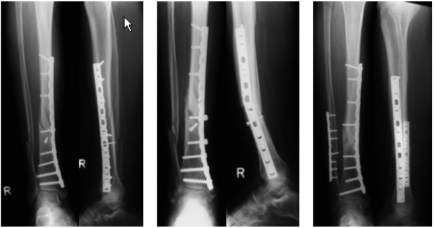
Plate osteosynthesis is one treatment option for the stabilization of long bones. It is widely accepted to achieve bone healing with a dynamic and biological fixation where the perfusion of the bone is left intact and micromotion at the fracture gap is allowed. The indications for a dynamic plate osteosynthesis include distal tibial and femoral fractures, some midshaft fractures, and adolescent tibial and femoral fractures with not fully closed growth plates. Although many lower limb shaft fractures are managed successfully with intramedullary nails, there are some important advantages of open-reduction-and-plate fixation: the risk of malalignment, anterior knee pain, or nonunion seems to be lower. The surgeon performing a plate osteosynthesis has the possibility to influence fixation strength and micromotion at the fracture gap. Long plates and oblique screws at the plate ends increase fixation strength. However, the number of screws does influence stiffness and stability. Lag screws and screws close to the fracture site reduce micromotion dramatically.DYNAMIC PLATE OSTEOSYNTHESIS CAN BE ACHIEVED BY APPLYING SOME SIMPLE RULES: long plates with only a few screws should be used. Oblique screws at the plate ends increase the pullout strength. Two or three holes at the fracture site should be omitted. Lag screws, especially through the plate, must be avoided whenever possible. Compression is not required. Locking plates are recommended only in fractures close to the joint. When respecting these basic concepts, dynamic plate osteosynthesis is a safe procedure with a high healing and a low complication rate.
钢板内固定是长骨稳定的一种治疗选择。通过动态生物固定实现骨愈合已被广泛接受,即保持骨的血供完整,并允许骨折间隙存在微动。动态钢板内固定的适应证包括胫骨干远端和股骨干骨折、一些骨干中段骨折以及生长板未完全闭合的青少年胫骨干和股骨干骨折。虽然许多下肢骨干骨折采用髓内钉治疗取得了成功,但切开复位钢板固定有一些重要优点:畸形、膝前疼痛或骨不连的风险似乎较低。进行钢板内固定的外科医生有可能影响骨折间隙的固定强度和微动。长钢板和钢板两端的斜形螺钉可增加固定强度。然而,螺钉数量确实会影响刚度和稳定性。拉力螺钉和靠近骨折部位的螺钉可显著减少微动。遵循一些简单规则即可实现动态钢板内固定:应使用螺钉数量少的长钢板。钢板两端的斜形螺钉可增加拔出强度。骨折部位应省略两三个螺孔。应尽可能避免使用拉力螺钉,尤其是穿过钢板的拉力螺钉。不需要加压。仅在靠近关节的骨折中推荐使用锁定钢板。遵循这些基本概念时,动态钢板内固定是一种安全的手术方法,愈合率高且并发症发生率低。