Department of Anaesthesiology and Intensive Care, Stavanger University Hospital, Stavanger, Norway.
Scand J Trauma Resusc Emerg Med. 2011 Aug 9;19:46. doi: 10.1186/1757-7241-19-46.
The aim of this study was to measure chest compression decay during simulated advanced life support (ALS) in a cardiac arrest manikin model.
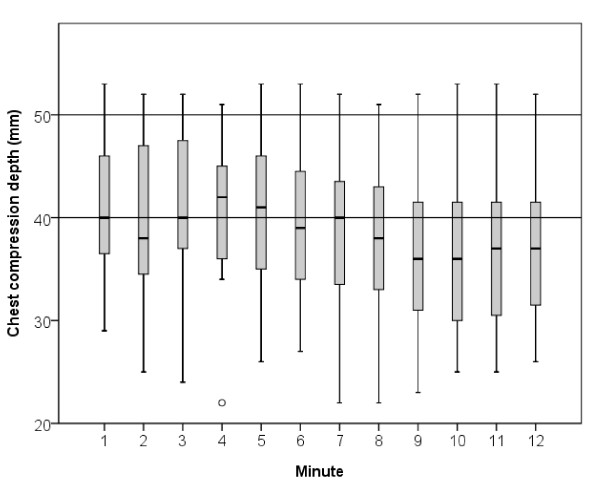
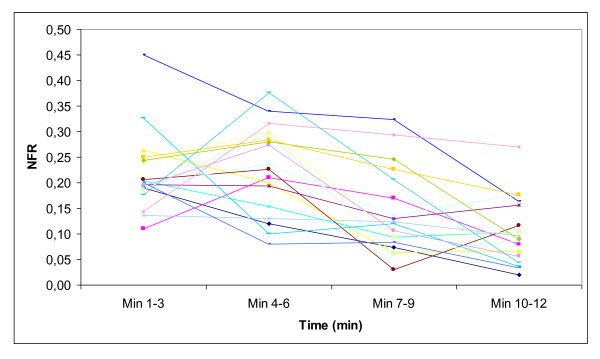
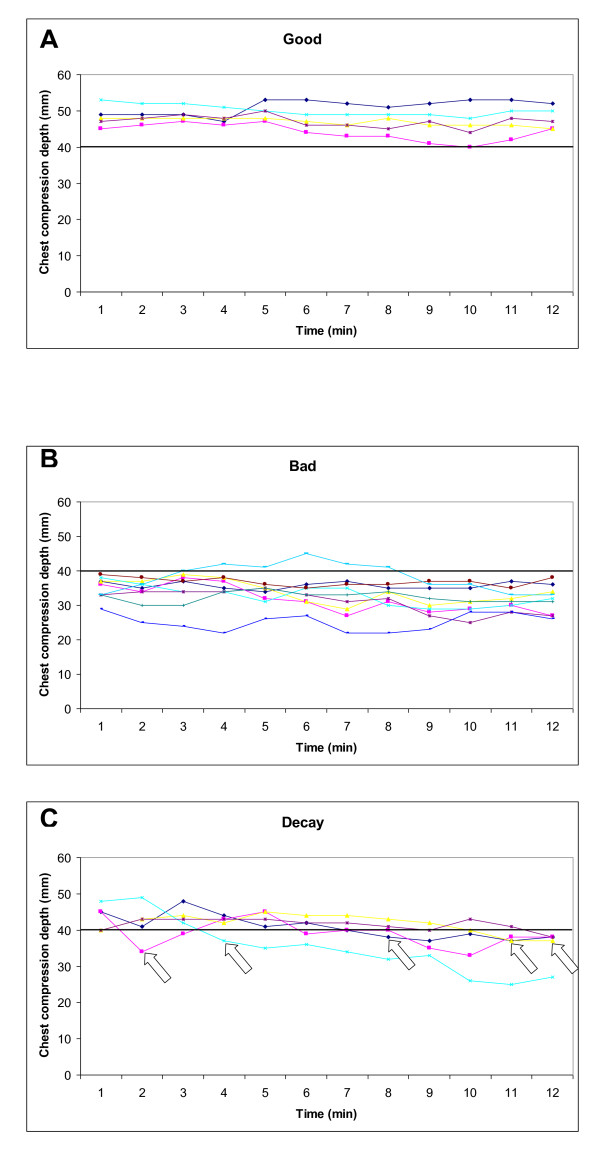
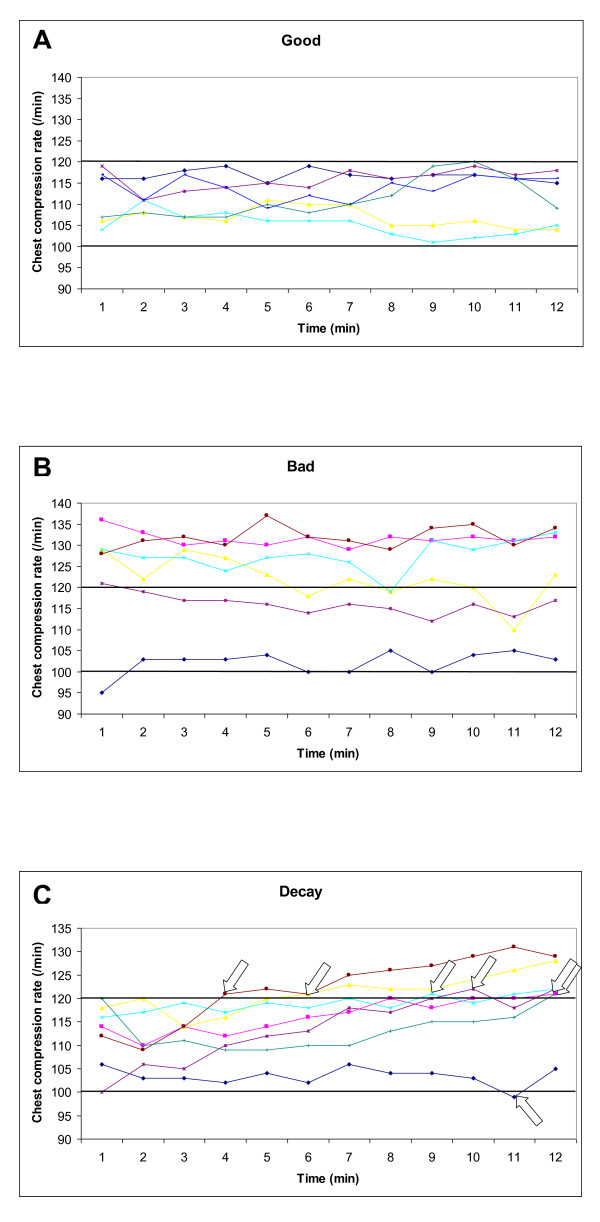
19 paramedic teams, each consisting of three paramedics, performed ALS for 12 minutes with the same paramedic providing all chest compressions. The patient was a resuscitation manikin found in ventricular fibrillation (VF). The first shock terminated the VF and the patient remained in pulseless electrical activity (PEA) throughout the scenario. Average chest compression depth and rate was measured each minute for 12 minutes and divided into three groups based on chest compression quality; good (compression depth ≥ 40 mm, compression rate 100-120/minute for each minute of CPR), bad (initial compression depth < 40 mm, initial compression rate < 100 or > 120/minute) or decay (change from good to bad during the 12 minutes). Changes in no-flow ratio (NFR, defined as the time without chest compressions divided by the total time of the ALS scenario) over time was also measured.
Based on compression depth, 5 (26%), 9 (47%) and 5 (26%) were good, bad and with decay, respectively. Only one paramedic experienced decay within the first two minutes. Based on compression rate, 6 (32%), 6 (32%) and 7 (37%) were good, bad and with decay, respectively. NFR was 22% in both the 1-3 and 4-6 minute periods, respectively, but decreased to 14% in the 7-9 minute period (P = 0.002) and to 10% in the 10-12 minute period (P < 0.001).
In this simulated cardiac arrest manikin study, only half of the providers achieved guideline recommended compression depth during prolonged ALS. Large inter-individual differences in chest compression quality were already present from the initiation of CPR. Chest compression decay and thereby fatigue within the first two minutes was rare.
本研究旨在测量在心脏骤停模型中模拟高级生命支持(ALS)期间的胸外按压衰减。
19 个急救小组,每组由 3 名急救人员组成,每个小组均对患者进行了 12 分钟的 ALS 治疗,且所有的胸外按压均由同一名急救人员提供。患者为处于室颤(VF)状态的复苏模型。首次电击终止了 VF,整个场景中患者一直处于无脉电活动(PEA)状态。在 12 分钟内,每分钟测量一次平均胸外按压深度和频率,并根据胸外按压质量将其分为三组;良好(按压深度≥40mm,每分钟按压频率 100-120 次)、不良(初始按压深度<40mm,初始按压频率<100 次或>120 次/分钟)或衰减(在 12 分钟内从良好变为不良)。还测量了无血流比(NFR,定义为无按压时间与 ALS 场景总时间的比值)随时间的变化。
根据按压深度,良好、不良和衰减分别为 5 例(26%)、9 例(47%)和 5 例(26%)。只有一名急救人员在前两分钟内出现衰减。根据按压频率,良好、不良和衰减分别为 6 例(32%)、6 例(32%)和 7 例(37%)。1-3 分钟和 4-6 分钟期间的 NFR 分别为 22%,但在 7-9 分钟期间降至 14%(P=0.002),在 10-12 分钟期间降至 10%(P<0.001)。
在这项模拟心脏骤停模型的研究中,只有一半的提供者在长时间的 ALS 期间达到了指南推荐的按压深度。从 CPR 开始时,胸外按压质量就存在较大的个体间差异。在前两分钟内,胸外按压衰减(从而导致疲劳)很少见。