Mycotic Diseases Branch, National Center for Emerging and Zoonotic Infectious Diseases, Centers for Disease Control and Prevention, Atlanta, Georgia, United States of America.
PLoS One. 2011;6(8):e23158. doi: 10.1371/journal.pone.0023158. Epub 2011 Aug 15.
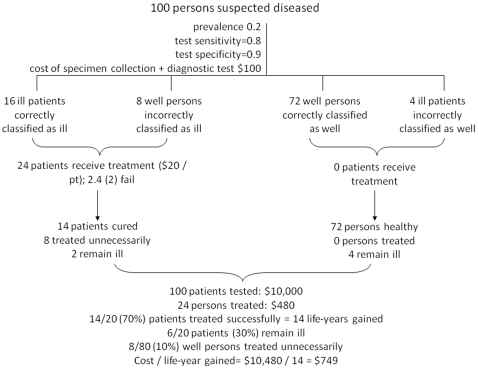
Diagnosis of Pneumocystis jirovecii pneumonia (PCP) is challenging, particularly in developing countries. Highly sensitive diagnostic methods are costly, while less expensive methods often lack sensitivity or specificity. Cost-effectiveness comparisons of the various diagnostic options have not been presented.
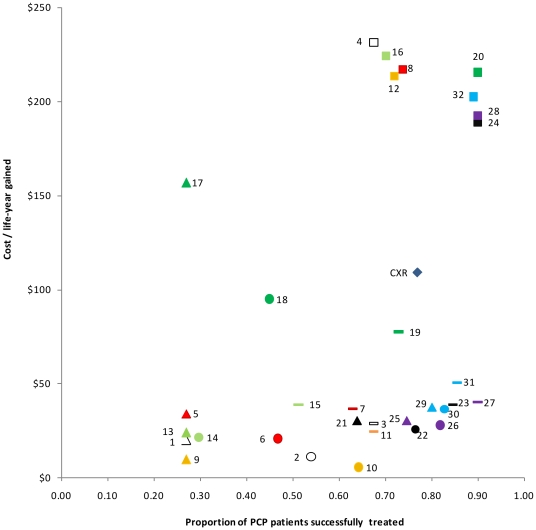
We compared cost-effectiveness, as measured by cost per life-years gained and proportion of patients successfully diagnosed and treated, of 33 PCP diagnostic options, involving combinations of specimen collection methods [oral washes, induced and expectorated sputum, and bronchoalveolar lavage (BAL)] and laboratory diagnostic procedures [various staining procedures or polymerase chain reactions (PCR)], or clinical diagnosis with chest x-ray alone. Our analyses were conducted from the perspective of the government payer among ambulatory, HIV-infected patients with symptoms of pneumonia presenting to HIV clinics and hospitals in South Africa. Costing data were obtained from the National Institutes of Communicable Diseases in South Africa. At 50% disease prevalence, diagnostic procedures involving expectorated sputum with any PCR method, or induced sputum with nested or real-time PCR, were all highly cost-effective, successfully treating 77-90% of patients at $26-51 per life-year gained. Procedures using BAL specimens were significantly more expensive without added benefit, successfully treating 68-90% of patients at costs of $189-232 per life-year gained. A relatively cost-effective diagnostic procedure that did not require PCR was Toluidine Blue O staining of induced sputum ($25 per life-year gained, successfully treating 68% of patients). Diagnosis using chest x-rays alone resulted in successful treatment of 77% of patients, though cost-effectiveness was reduced ($109 per life-year gained) compared with several molecular diagnostic options.
For diagnosis of PCP, use of PCR technologies, when combined with less-invasive patient specimens such as expectorated or induced sputum, represent more cost-effective options than any diagnostic procedure using BAL, or chest x-ray alone.
肺孢子菌肺炎(PCP)的诊断具有挑战性,尤其是在发展中国家。高灵敏度的诊断方法成本高昂,而较便宜的方法通常缺乏灵敏度或特异性。尚未对各种诊断选择的成本效益进行比较。
我们比较了 33 种 PCP 诊断方案的成本效益,这些方案涉及标本采集方法(口腔冲洗、诱导和咳出的痰液以及支气管肺泡灌洗(BAL))和实验室诊断程序(各种染色程序或聚合酶链反应(PCR))的组合,或单独使用胸部 X 射线进行临床诊断。我们的分析是从南非门诊、感染 HIV 的肺炎症状出现于 HIV 诊所和医院的政府支付者的角度进行的。成本数据来自南非国家传染病研究所。在 50%疾病流行率的情况下,涉及任何 PCR 方法的咳出痰液或巢式或实时 PCR 的诱导痰液的诊断程序都具有很高的成本效益,以 26-51 美元/生命年的成本成功治疗了 77-90%的患者。使用 BAL 标本的程序成本更高,但没有额外的益处,以 189-232 美元/生命年的成本成功治疗了 68-90%的患者。一种相对具有成本效益的诊断程序,不需要 PCR,即甲苯胺蓝 O 染色诱导的痰液(25 美元/生命年,成功治疗 68%的患者)。单独使用胸部 X 射线进行诊断可使 77%的患者得到成功治疗,尽管与几种分子诊断选择相比,成本效益降低(每获得 1 个生命年需花费 109 美元)。
对于 PCP 的诊断,使用 PCR 技术,与 BAL 或单独使用胸部 X 射线相比,与侵袭性较小的患者标本(如咳出的或诱导的痰液)结合使用时,代表更具成本效益的选择。