Department of Anesthesiology and Pain Medicine, Seoul National University Bundang Hospital, Seoul, Korea.
Korean J Anesthesiol. 2011 Jul;61(1):12-8. doi: 10.4097/kjae.2011.61.1.12. Epub 2011 Jul 21.
With ultrasound guidance, the success rate of brachial plexus block (BPB) is 95-100% and the anesthetic time has become a more important factor than before. Many investigators have compared ultrasound guidance with the nerve stimulation technique, but there are few studies comparing different approaches via the same ultrasound guidance. We compared the axillary BPB with the infraclavicular BPB under ultrasound guidance.
Twenty-two ASA physical status I-II patients presenting with elective forearm surgery were prospectively randomized to receive an axillary BPB (group AX) or an infraclavicular BPB (group IC) with ultrasound guidance. Both groups received a total of 20 ml of 1.5% lidocaine with 5 µg/ml epinephrine and 0.1 mEq/ml sodium bicarbonate. Patients were then evaluated for block onset and block performance time was also recorded.
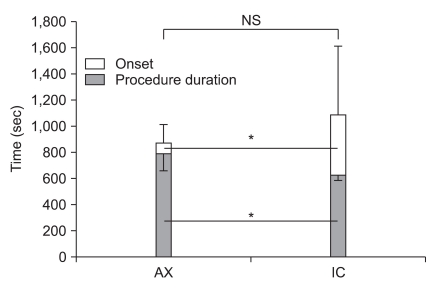
Group IC demonstrated a reduction in performance time vs. group AX (622 ± 139 sec vs. 789 ± 131 sec, P < 0.05). But, the onset time was longer in group IC than in group AX (7.7 ± 8.8 min vs. 1.4 ± 2.3 min, P < 0.05). All blocks were successful in both groups.
Under ultrasound guidance, infraclavicular BPB was faster to perform than the axillary approach. But the block onset was slower with the infraclavicular approach.
在超声引导下,臂丛神经阻滞(BPB)的成功率为 95-100%,麻醉时间已成为比以往更为重要的因素。许多研究人员比较了超声引导与神经刺激技术,但比较相同超声引导下不同方法的研究较少。我们比较了超声引导下腋路和锁骨下入路臂丛神经阻滞。
22 例 ASA Ⅰ-Ⅱ级拟行前臂手术的患者前瞻性随机分为腋路臂丛神经阻滞组(AX 组)或锁骨下入路臂丛神经阻滞组(IC 组),均采用超声引导。两组均给予 20ml 1.5%利多卡因加 5μg/ml 肾上腺素和 0.1mEq/ml 碳酸氢钠。然后评估阻滞起效时间,并记录阻滞起效时间。
IC 组的阻滞起效时间短于 AX 组(7.7±8.8min 比 1.4±2.3min,P<0.05),但阻滞起效时间长于 AX 组(622±139sec 比 789±131sec,P<0.05)。两组阻滞均成功。
在超声引导下,锁骨下入路臂丛神经阻滞起效更快,但锁骨下入路阻滞起效更慢。