Department of Cardiothoracic Surgery, Boston Medical Center, 88 East Newton Street, Boston, MA 02118, USA.
J Thorac Cardiovasc Surg. 2011 Nov;142(5):1143-51. doi: 10.1016/j.jtcvs.2011.07.051. Epub 2011 Aug 26.
Sublobar resection (SR) is commonly used for patients considered high risk for lobectomy. Nonoperative therapies are increasingly being reported for patients with similar risk because of perceived lower morbidity. We report 30- and 90-day adverse events (AEs) from American College of Surgeons Oncology Group Z4032, a multicenter phase III study for high-risk patients with stage I non-small cell lung cancer.
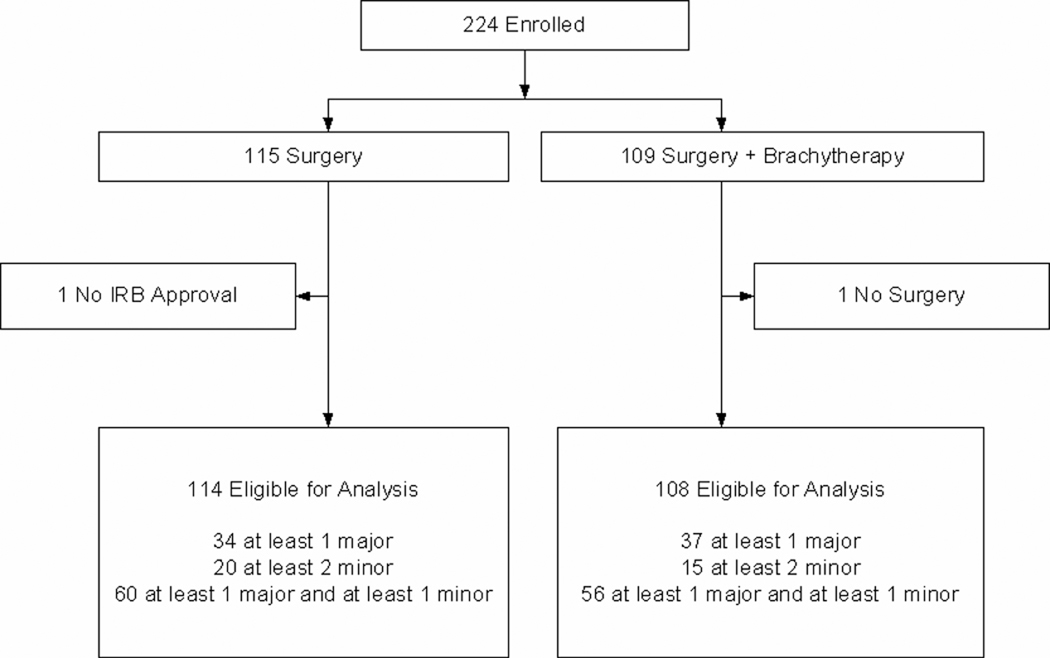
Data from 222 evaluable patients randomized to SR (n = 114) or SR with brachytherapy (n = 108) are reported. AEs were recorded using the Common Terminology Criteria for Adverse Events, Version 3.0, at 30 and 90 days after surgery. Risk factors (age, percent baseline carbon monoxide diffusion in the lung [DLCO%], percent forced expiratory volume in 1 second [FEV1%], upper lobe vs lower lobe resections, performance status, surgery approach, video-assisted thoracic surgery vs open and extent, and wedge vs segmentectomy) were analyzed using a multivariable logistic model for their impact on the incidence of grade 3 or higher (G3+) AEs. Respiratory AEs were also specifically analyzed.
Median age, FEV1%, and DLCO% were similar in the 2 treatment groups. There was no difference in the location of resection (upper vs lower lobe) or the use of segmental or wedge resections. There were no differences between the groups with respect to "respiratory" G3+ AEs (30 days: 14.9% vs 19.4%, P = .35; 0-90 days: 19.3% vs 25%, P = .31) and "any" G3+ AEs (30 days: 25.4% vs 30.6%, P = .37; 0-90 days: 29.8% vs 37%, P = .25). Further analysis combined the 2 groups. Mortality occurred in 3 patients (1.4%) by 30 days and in 6 patients (2.7%) by 90 days. Four of the 6 deaths were thought to be due to surgery. When considered as continuous variables, FEV1% was associated with "any" G3+ AE at days 0 to 30 (P = .03; odds ratio [OR] = 0.98) and days 0 to 90 (P = .05; OR = 0.98), and DLCO% was associated with "respiratory" G3+ AE at days 0 to 30 (P = .03; OR = 0.97) and days 0 to 90 (P = .05; OR = 0.98). Segmental resection was associated with a higher incidence of any G3+ AE compared with wedge resection at days 0 to 30 (40.3% vs 22.7%; OR = 2.56; P < .01) and days 0 to 90 (41.5% vs 29.7%; OR = 1.96; P = .04). The median FEV1% was 50%, and the median DLCO% was 46%. By using these median values as potential cutpoints, only a DLCO% of less than 46% was significantly associated with an increased risk of "respiratory" and "any" G3+ AE for days 0 to 30 and 0 to 90.
In a multicenter setting, SR with brachytherapy was not associated with increased morbidity compared with SR alone. SR/SR with brachytherapy can be performed safely in high-risk patients with non-small cell lung cancer with low 30- and 90-day mortality and acceptable morbidity. Segmental resection was associated with increased "any" G3+ AE, and DLCO% less than 46% was associated with "any" G3+ AE and "respiratory" G3+ AE at both 30 and 90 days.
对于被认为行肺叶切除术风险较高的患者,亚肺叶切除术(SR)通常被采用。由于认为发病率较低,越来越多的非手术治疗方法也被用于具有相似风险的患者。我们报告了美国外科医师学院肿瘤学组 Z4032 的 30 天和 90 天不良事件(AE)数据,这是一项针对 I 期非小细胞肺癌高危患者的多中心 III 期研究。
报告了 222 例可评估患者的数据,这些患者随机分为 SR(n = 114)或 SR 加近距离放疗(n = 108)组。术后 30 天和 90 天使用通用术语标准(CTCAE)版本 3.0 记录 AE。使用多变量逻辑模型分析年龄、肺一氧化碳弥散量百分比(DLCO%)、用力呼气量第一秒百分比(FEV1%)、上叶或下叶切除术、表现状态、手术入路、电视辅助胸腔镜手术与开胸手术和范围、楔形切除术与节段切除术等风险因素对 3 级或更高(G3+)AE 发生率的影响。还专门分析了呼吸系统 AE。
两组的中位年龄、FEV1%和 DLCO%相似。切除术的部位(上叶与下叶)或使用的节段或楔形切除术没有差异。两组之间在“呼吸系统”G3+AE(30 天:14.9%比 19.4%,P =.35;0-90 天:19.3%比 25%,P =.31)和“任何”G3+AE(30 天:25.4%比 30.6%,P =.37;0-90 天:29.8%比 37%,P =.25)方面无差异。进一步分析将两组合并。30 天内有 3 例(1.4%)患者死亡,90 天内有 6 例(2.7%)患者死亡。6 例死亡中有 4 例被认为与手术有关。当考虑为连续变量时,FEV1%与 0 至 30 天(P =.03;比值比[OR] = 0.98)和 0 至 90 天(P =.05;OR = 0.98)的“任何”G3+AE 相关,DLCO%与 0 至 30 天(P =.03;OR = 0.97)和 0 至 90 天(P =.05;OR = 0.98)的“呼吸系统”G3+AE 相关。与楔形切除术相比,节段切除术在 0 至 30 天(40.3%比 22.7%;OR = 2.56;P <.01)和 0 至 90 天(41.5%比 29.7%;OR = 1.96;P =.04)时与任何 G3+AE 的发生率较高。中位 FEV1%为 50%,中位 DLCO%为 46%。使用这些中位数作为潜在的截断值,仅 DLCO%低于 46%与 0 至 30 天和 0 至 90 天的“呼吸系统”和“任何”G3+AE 风险增加显著相关。
在多中心环境中,SR 加近距离放疗与单独 SR 相比,发病率无增加。SR/SR 加近距离放疗可安全用于高危非小细胞肺癌患者,30 天和 90 天死亡率低,发病率可接受。节段切除术与任何 G3+AE 发生率增加相关,DLCO%低于 46%与 30 天和 90 天的任何 G3+AE 和“呼吸系统”G3+AE 相关。