Departamento de Saúde Coletiva, Universidade de Brasília, Campus Universitário Darcy Ribeiro, CEP 70910-900, Brasília, DF, Brazil.
Health Res Policy Syst. 2011 Aug 31;9:35. doi: 10.1186/1478-4505-9-35.
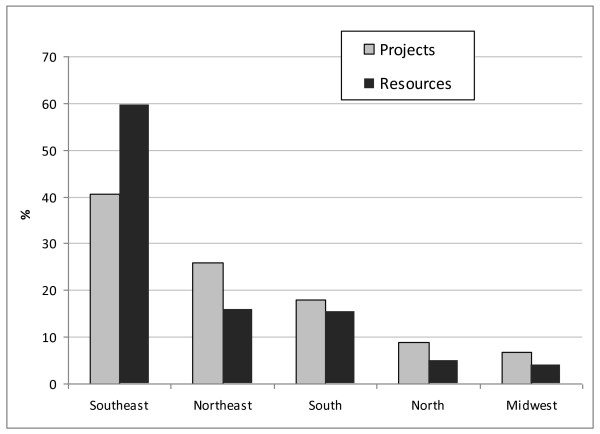
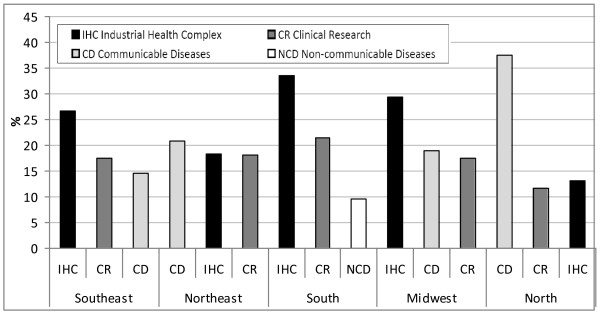
This commentary describes how the Brazilian Ministry of Health's (MoH) research support policy fulfilled the National Agenda of Priorities in Health Research (NAPHR). In 2003, the MoH started a democratic process in order to establish a priority agenda in health research involving investigators, health managers and community leaders. The Agenda was launched in 2004 and is guiding budget allocations in an attempt to reduce the gap between scientific knowledge and health practice and activities, aiming to contribute to improving Brazilian quality of life. Many strategies were developed, for instance: Cooperation Agreements between the Ministry of Health and the Ministry of Science and Technology; the decentralization of research support at state levels with the participation of local Health Secretariats and Science and Technology Institutions; Health Technology Assessment; innovation in neglected diseases; research networks and multicenter studies in adult, women's and children's health; cardiovascular risk in adolescents; clinical research and stem cell therapy. The budget allocated by the Ministry of Health and partners was expressive: US$419 million to support almost 3,600 projects. The three sub-agenda with the higher proportion of resources were "industrial health complex", "clinical research" and "communicable diseases", which are considered strategic for innovation and national development. The Southeast region conducted 40.5% of all projects and detained 59.7% of the resources, attributable to the concentration of the most traditional health research institutes and universities in the states of São Paulo and Rio de Janeiro. The second most granted region was the Northeast, which reflects the result of a governmental policy to integrate and modernize this densely populated area and the poorest region in the country. Although Brazil began the design and implementation of the NAPHR in 2003, it has done so in accordance with the 'good practice principles' recently published: inclusive process, information gathering, careful planning and funding policy, transparency and internal evaluation (an external independent evaluation is underway). The effort in guiding the health research policy has achieved and legitimated an unprecedented developmental spurt to support strategic health research. We believe this experience is valuable and applicable to other countries, but different settings and local political circumstances will determine the best course of action to follow.
这篇评论描述了巴西卫生部(MoH)的研究支持政策如何实现国家卫生研究优先议程(NAPHR)。2003 年,MoH 开始了一个民主进程,以便在卫生研究中确立一个涉及调查人员、卫生管理人员和社区领导人的优先议程。该议程于 2004 年启动,指导预算分配,试图缩小科学知识与卫生实践和活动之间的差距,旨在为改善巴西生活质量做出贡献。制定了许多战略,例如:卫生部与科学技术部之间的合作协议;在地方卫生部门和科学技术机构参与下,将研究支持权力下放;卫生技术评估;创新治疗被忽视的疾病;研究网络和成人、妇女和儿童健康的多中心研究;青少年心血管风险;临床研究和干细胞治疗。卫生部和合作伙伴分配的预算是可观的:4.19 亿美元用于支持近 3600 个项目。资源比例最高的三个分议程是“工业卫生综合体”、“临床研究”和“传染病”,它们被认为是创新和国家发展的战略。东南部地区完成了所有项目的 40.5%,占资源的 59.7%,这归因于该地区集中了最传统的卫生研究机构和大学,位于圣保罗和里约热内卢州。获得资助第二多的地区是东北部,这反映了政府整合和现代化这个人口稠密且是全国最贫穷地区的政策结果。尽管巴西于 2003 年开始设计和实施 NAPHR,但它是根据最近发布的“良好实践原则”进行的:包容的过程、信息收集、精心规划和资助政策、透明度和内部评估(正在进行外部独立评估)。引导卫生研究政策的努力取得了前所未有的发展势头,为支持战略卫生研究提供了合法性。我们认为,这种经验是有价值的,适用于其他国家,但不同的背景和当地政治情况将决定采取的最佳行动方案。