Treggiari Miriam M, Retsch-Bogart George, Mayer-Hamblett Nicole, Khan Umer, Kulich Michal, Kronmal Richard, Williams Judy, Hiatt Peter, Gibson Ronald L, Spencer Terry, Orenstein David, Chatfield Barbara A, Froh Deborah K, Burns Jane L, Rosenfeld Margaret, Ramsey Bonnie W
Department of Anesthesiology and Pain Medicine, Seattle Children’s Hospital, WA 98104, USA.
Arch Pediatr Adolesc Med. 2011 Sep;165(9):847-56. doi: 10.1001/archpediatrics.2011.136.
To investigate the efficacy and safety of 4 antipseudomonal treatments in children with cystic fibrosis with recently acquired Pseudomonas aeruginosa infection.
Randomized controlled trial.
Multicenter trial in the United States.
Three hundred four children with cystic fibrosis aged 1 to 12 years within 6 months of P aeruginosa detection.
Participants were randomized to 1 of 4 antibiotic regimens for 18 months (six 12-week quarters) between December 2004 and June 2009. Participants randomized to cycled therapy received tobramycin inhalation solution (300 mg twice a day) for 28 days, with oral ciprofloxacin (15-20 mg/kg twice a day) or oral placebo for 14 days every quarter, while participants randomized to culture-based therapy received the same treatments only during quarters with positive P aeruginosa cultures.
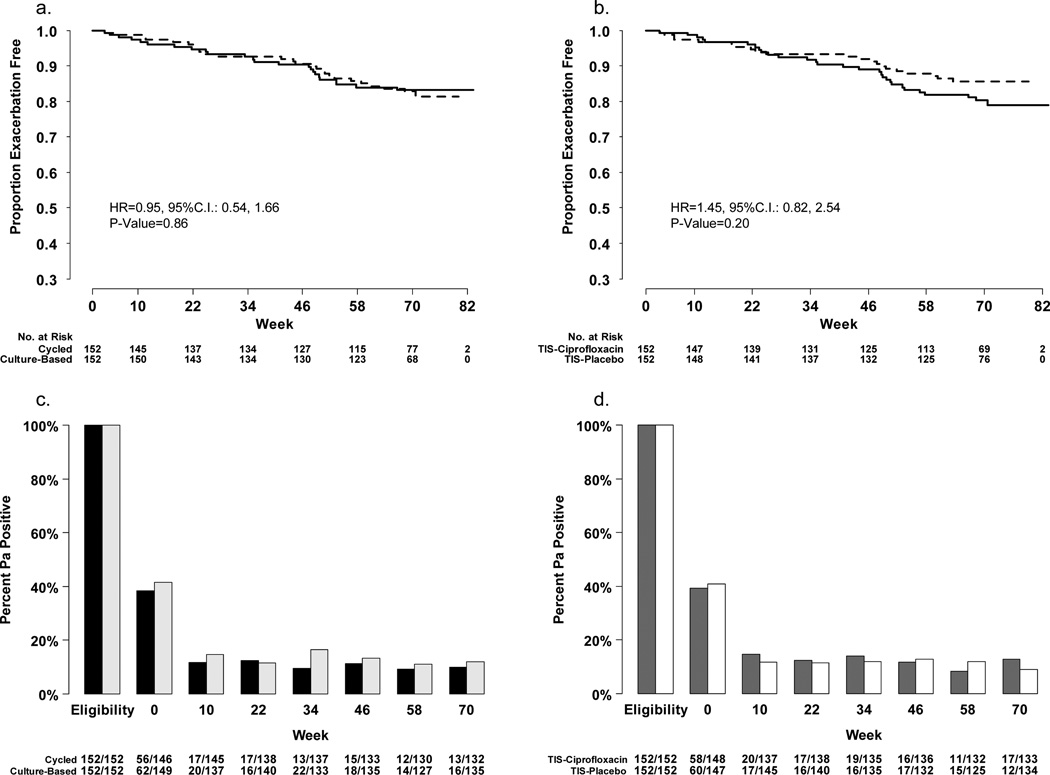
The primary end points were time to pulmonary exacerbation requiring intravenous antibiotics and proportion of P aeruginosa -positive cultures.
The intention-to-treat analysis included 304 participants. There was no interaction between treatments. There were no statistically significant differences in exacerbation rates between cycled and culture-based groups (hazard ratio, 0.95; 95% confidence interval [CI], 0.54-1.66) or ciprofloxacin and placebo (hazard ratio, 1.45; 95% CI, 0.82-2.54). The odds ratios of P aeruginosa- positive culture comparing the cycled vs culture-based group were 0.78 (95% CI, 0.49-1.23) and 1.10 (95% CI, 0.71-1.71) comparing ciprofloxacin vs placebo. Adverse events were similar across groups.
No difference in the rate of exacerbation or prevalence of P aeruginosa positivity was detected between cycled and culture-based therapies. Adding ciprofloxacin produced no benefits.
ClinicalTrials.gov Identifier: NCT00097773.
探讨4种抗铜绿假单胞菌治疗方案对近期感染铜绿假单胞菌的囊性纤维化患儿的疗效和安全性。
随机对照试验。
美国的多中心试验。
304名年龄在1至12岁之间、在检测到铜绿假单胞菌后6个月内的囊性纤维化患儿。
2004年12月至2009年6月期间,参与者被随机分配到4种抗生素治疗方案中的一种,为期18个月(六个12周的季度)。随机接受循环治疗的参与者每季度接受28天的妥布霉素吸入溶液(每日两次,每次300毫克)治疗,并口服环丙沙星(每日两次,每次15 - 20毫克/千克)或口服安慰剂14天,而随机接受基于培养的治疗的参与者仅在铜绿假单胞菌培养阳性的季度接受相同治疗。
主要终点为需要静脉使用抗生素的肺部加重时间和铜绿假单胞菌阳性培养比例。
意向性分析纳入304名参与者。各治疗组之间无交互作用。循环治疗组和基于培养的治疗组之间的加重率无统计学显著差异(风险比,0.95;95%置信区间[CI],0.54 - 1.66),环丙沙星组和安慰剂组之间也无显著差异(风险比,1.45;95% CI,0.82 - 2.54)。循环治疗组与基于培养的治疗组相比,铜绿假单胞菌阳性培养的比值比为0.78(95% CI,0.49 - 1.23),环丙沙星组与安慰剂组相比为1.10(95% CI,0.71 - 1.71)。各组不良事件相似。
循环治疗和基于培养的治疗在加重率或铜绿假单胞菌阳性率方面未发现差异。添加环丙沙星无益处。
ClinicalTrials.gov标识符:NCT00097773。