Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD 21205, USA.
BMC Public Health. 2011 Sep 18;11:704. doi: 10.1186/1471-2458-11-704.
Physicians involved in primary prevention are key players in CVD risk control strategies, but the expected reduction in CVD risk that would be obtained if all patients attending primary care had their risk factors controlled according to current guidelines is unknown. The objective of this study was to estimate the excess risk attributable, firstly, to the presence of CVD risk factors and, secondly, to the lack of control of these risk factors in primary prevention care across Europe.
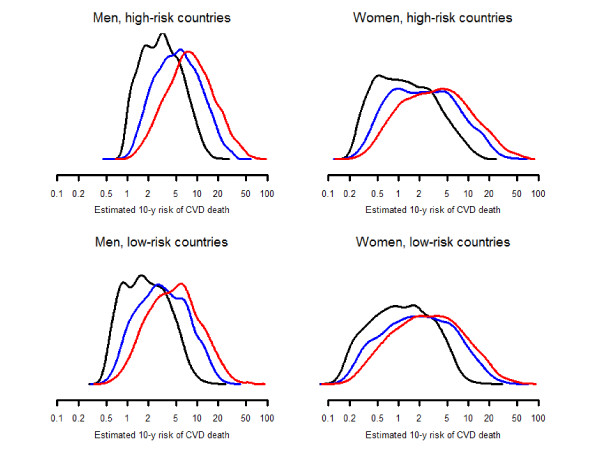
Cross-sectional study using data from the European Study on Cardiovascular Risk Prevention and Management in Daily Practice (EURIKA), which involved primary care and outpatient clinics involved in primary prevention from 12 European countries between May 2009 and January 2010. We enrolled 7,434 patients over 50 years old with at least one cardiovascular risk factor but without CVD and calculated their 10-year risk of CVD death according to the SCORE equation, modified to take diabetes risk into account.
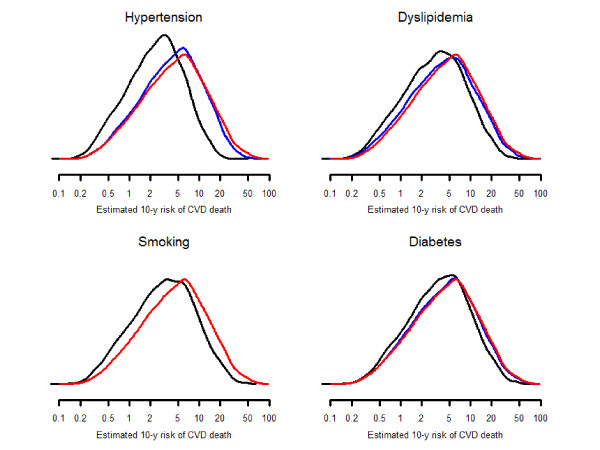
The average 10-year risk of CVD death in study participants (N = 7,434) was 8.2%. Hypertension, hyperlipidemia, smoking, and diabetes were responsible for 32.7 (95% confidence interval 32.0-33.4), 15.1 (14.8-15.4), 10.4 (9.9-11.0), and 16.4% (15.6-17.2) of CVD risk, respectively. The four risk factors accounted for 57.7% (57.0-58.4) of CVD risk, representing a 10-year excess risk of CVD death of 5.66% (5.47-5.85). Lack of control of hypertension, hyperlipidemia, smoking, and diabetes were responsible for 8.8 (8.3-9.3), 10.6 (10.3-10.9), 10.4 (9.9-11.0), and 3.1% (2.8-3.4) of CVD risk, respectively. Lack of control of the four risk factors accounted for 29.2% (28.5-29.8) of CVD risk, representing a 10-year excess risk of CVD death of 3.12% (2.97-3.27).
Lack of control of CVD risk factors was responsible for almost 30% of the risk of CVD death among patients participating in the EURIKA Study.
参与初级预防的医生是 CVD 风险控制策略的关键参与者,但如果所有接受初级保健的患者都按照当前指南控制其风险因素,那么预期可以降低多少 CVD 风险尚不清楚。本研究的目的是首先估计 CVD 风险因素的存在以及其次,在欧洲初级预防护理中,这些风险因素控制不佳会导致多少额外风险。
这是一项使用 2009 年 5 月至 2010 年 1 月期间来自欧洲心血管风险预防和管理日常实践研究(EURIKA)的数据进行的横断面研究,该研究涉及 12 个欧洲国家的初级保健和门诊诊所。我们招募了 7434 名年龄在 50 岁以上、至少有一个心血管风险因素但没有 CVD 的患者,并根据 SCORE 方程计算他们的 10 年 CVD 死亡风险,该方程经过修改以考虑糖尿病风险。
研究参与者(N=7434)的平均 10 年 CVD 死亡风险为 8.2%。高血压、高血脂、吸烟和糖尿病分别导致 32.7%(95%置信区间 32.0-33.4)、15.1%(14.8-15.4)、10.4%(9.9-11.0)和 16.4%(15.6-17.2)的 CVD 风险。这四个风险因素占 CVD 风险的 57.7%(57.0-58.4),代表 10 年 CVD 死亡的超额风险为 5.66%(5.47-5.85)。高血压、高血脂、吸烟和糖尿病控制不佳分别导致 8.8%(8.3-9.3)、10.6%(10.3-10.9)、10.4%(9.9-11.0)和 3.1%(2.8-3.4)的 CVD 风险。这四个风险因素控制不佳占 CVD 风险的 29.2%(28.5-29.8),代表 10 年 CVD 死亡的超额风险为 3.12%(2.97-3.27)。
EURIKA 研究参与者中 CVD 风险因素控制不佳导致近 30%的 CVD 死亡风险。