Department of Anesthesiology and Intensive Care Medicine, Northern State Medical University, Troitsky avenue 51, Arkhangelsk, 163000, Russian Federation.
BMC Anesthesiol. 2011 Sep 18;11:17. doi: 10.1186/1471-2253-11-17.
Our aim was to assess the efficacy of thoracic epidural anesthesia (EA) followed by postoperative epidural infusion (EI) and patient-controlled epidural analgesia (PCEA) with ropivacaine/fentanyl in off-pump coronary artery bypass grafting (OPCAB).
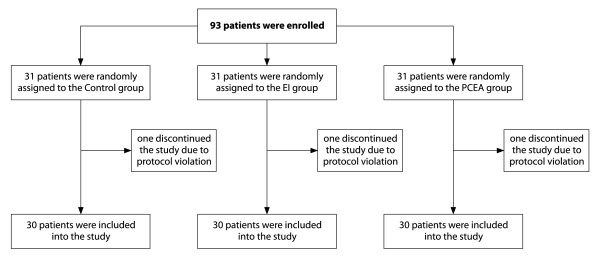
In a prospective study, 93 patients were scheduled for OPCAB under propofol/fentanyl anesthesia and randomized to three postoperative analgesia regimens aiming at a visual analog scale (VAS) score < 30 mm at rest. The control group (n = 31) received intravenous fentanyl 10 μg/ml postoperatively 3-8 mL/h. After placement of an epidural catheter at the level of Th2-Th4 before OPCAB, a thoracic EI group (n = 31) received EA intraoperatively with ropivacaine 0.75% 1 mg/kg and fentanyl 1 μg/kg followed by continuous EI of ropivacaine 0.2% 3-8 mL/h and fentanyl 2 μg/mL postoperatively. The PCEA group (n = 31), in addition to EA and EI, received PCEA (ropivacaine/fentanyl bolus 1 mL, lock-out interval 12 min) postoperatively. Hemodynamics and blood gases were measured throughout 24 h after OPCAB.
During OPCAB, EA decreased arterial pressure transiently, counteracted changes in global ejection fraction and accumulation of extravascular lung water, and reduced the consumption of propofol by 15%, fentanyl by 50% and nitroglycerin by a 7-fold, but increased the requirements in colloids and vasopressors by 2- and 3-fold, respectively (P < 0.05). After OPCAB, PCEA increased PaO2/FiO2 at 18 h and decreased the duration of mechanical ventilation by 32% compared with the control group (P < 0.05).
In OPCAB, EA with ropivacaine/fentanyl decreases arterial pressure transiently, optimizes myocardial performance and influences the perioperative fluid and vasoactive therapy. Postoperative EI combined with PCEA improves lung function and reduces time to extubation.
NCT01384175.
本研究旨在评估胸段硬膜外麻醉(EA)联合术后硬膜外输注(EI)和罗哌卡因/芬太尼病人自控硬膜外镇痛(PCEA)在非体外循环冠状动脉旁路移植术(OPCAB)中的疗效。
前瞻性研究,93 例行异丙酚/芬太尼麻醉下 OPCAB 的患者,随机分为三组,术后镇痛的目标是静息状态下视觉模拟评分(VAS)<30mm。对照组(n=31)术后接受芬太尼 10μg/ml,静脉推注 3-8ml/h。在 OPCAB 前于 Th2-Th4 水平放置硬膜外导管,EA 组(n=31)术中给予 0.75%罗哌卡因 1mg/kg 和芬太尼 1μg/kg,术后给予 0.2%罗哌卡因 3-8ml/h 和芬太尼 2μg/ml 持续 EI。PCEA 组(n=31)除 EA 和 EI 外,术后给予 PCEA(罗哌卡因/芬太尼 1ml 推注,锁定间隔 12min)。OPCAB 后 24 小时内监测血流动力学和血气。
OPCAB 期间,EA 使动脉压短暂下降,拮抗全心射血分数的变化和血管外肺水的蓄积,并使异丙酚、芬太尼和硝酸甘油的消耗分别减少 15%、50%和 7 倍,但胶体和血管加压药的需求分别增加 2 倍和 3 倍(P<0.05)。与对照组相比,术后 PCEA 使 PaO2/FiO2 在 18 小时增加,并使机械通气时间缩短 32%(P<0.05)。
OPCAB 中,罗哌卡因/芬太尼的 EA 使动脉压短暂下降,优化心肌功能,并影响围手术期液体和血管活性治疗。术后 EI 联合 PCEA 可改善肺功能并缩短拔管时间。
NCT01384175。