Manchester Royal Infirmary, M13 9WL Manchester, UK.
J Crit Care. 2012 Feb;27(1):89-94. doi: 10.1016/j.jcrc.2011.07.080. Epub 2011 Sep 29.
The aims of this study were to assess the feasibility of cardiopulmonary exercise testing (CPET) for the early assessment of cardiorespiratory fitness in general adult intensive care unit (ICU) survivors and to characterize the pathophysiology of exercise limitation in this population.
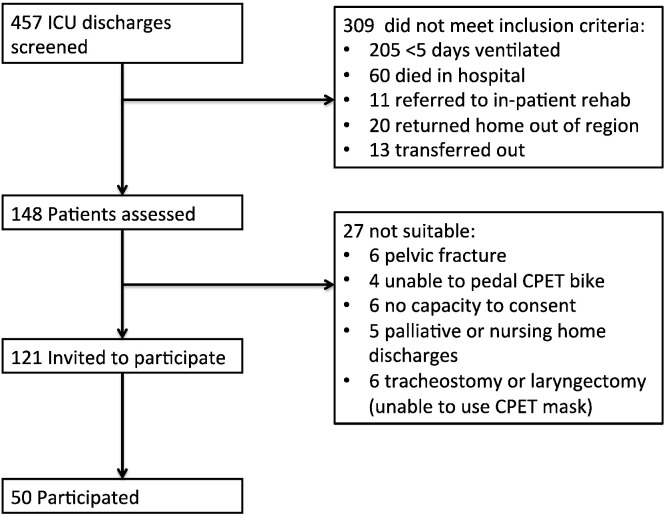
Fifty general ICU survivors (ventilated for ≥ 5 days) performed a maximal cycle ergometer CPET within 6 weeks of hospital discharge. Health-related quality of life was measured by the Medical Outcome Study Short Form 36 version 2.0 questionnaire.
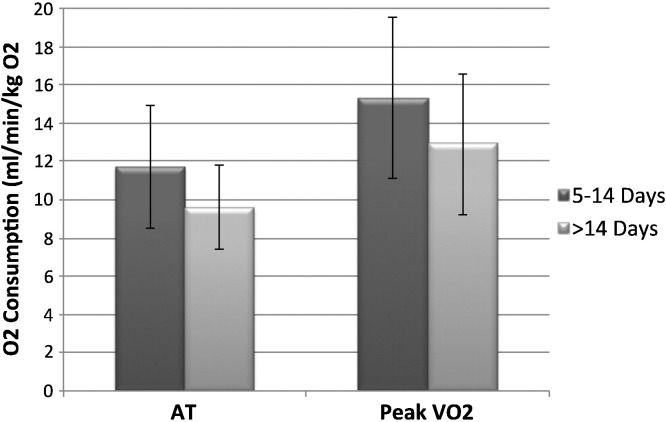
Fifty patients (median age, 57 years; median Acute Physiology And Chronic Health Evaluation II score, 16) completed a CPET 24 ± 14 days after hospital discharge with no adverse events. Significant exercise limitation was present with peak Vo(2) 56% ± 16% predicted and anaerobic threshold (AT) 41% ± 13% of peak predicted Vo(2). Prospectively stratified subgroup comparison showed that patients ventilated for 14 days or more had a significantly lower AT and peak Vo(2) than those ventilated for 5 to 14 days (AT: 9.6 vs 11.7 mL/kg per minute O(2), P = .009; peak Vo(2): 12.9 vs 15.3 mL/kg per minute O(2), P = .022). At peak exercise, heart rate reserve was 25% ± 14%, breathing reserve was 47% ± 19%, and the respiratory exchange ratio was 0.96 ± 0.11. Ventilatory equivalents for CO(2) (Eqco(2)) were 39 ± 9.
Significant exercise limitation is evident in patients who have had critical illness. Etiology of exercise limitation appears multifactorial, with general deconditioning and muscle weakness as major contributory factors. Early CPET appears a practical method of assessing exercise capacity in ICU survivors. Cardiopulmonary exercise testing could be used to select patients who may benefit most from a targeted physical rehabilitation program, aid in exercise prescription, and help assess the response to intervention.
本研究旨在评估心肺运动试验(CPET)在评估普通成人重症监护病房(ICU)幸存者心肺功能方面的可行性,并对该人群运动受限的病理生理学进行特征描述。
50 名 ICU 幸存者(机械通气≥5 天)在出院后 6 周内进行了最大的踏车 CPET。采用医疗结局研究短表 36 版本 2.0 问卷测量健康相关生活质量。
50 例患者(中位年龄,57 岁;急性生理学和慢性健康评估Ⅱ评分,16)在出院后 24±14 天完成了 CPET,无不良事件发生。存在显著的运动受限,峰值 Vo(2)为预测值的 56%±16%,无氧阈(AT)为预测峰值 Vo(2)的 41%±13%。前瞻性分层亚组比较显示,通气时间≥14 天的患者 AT 和峰值 Vo(2)明显低于通气时间为 5-14 天的患者(AT:9.6 比 11.7 mL/kg/min O(2),P=0.009;峰值 Vo(2):12.9 比 15.3 mL/kg/min O(2),P=0.022)。在峰值运动时,心率储备为 25%±14%,呼吸储备为 47%±19%,呼吸交换率为 0.96±0.11。CO(2)通气当量(Eqco(2))为 39±9。
危重病患者存在明显的运动受限。运动受限的病因似乎是多因素的,全身性去适应和肌肉无力是主要的促成因素。早期 CPET 似乎是评估 ICU 幸存者运动能力的实用方法。CPET 可用于选择最可能从有针对性的身体康复计划中受益的患者,辅助运动处方,并帮助评估干预的反应。