Modelling and Economics, Health Protection Agency, London NW9 5EQ, UK.
BMJ. 2011 Oct 5;343:d5694. doi: 10.1136/bmj.d5694.
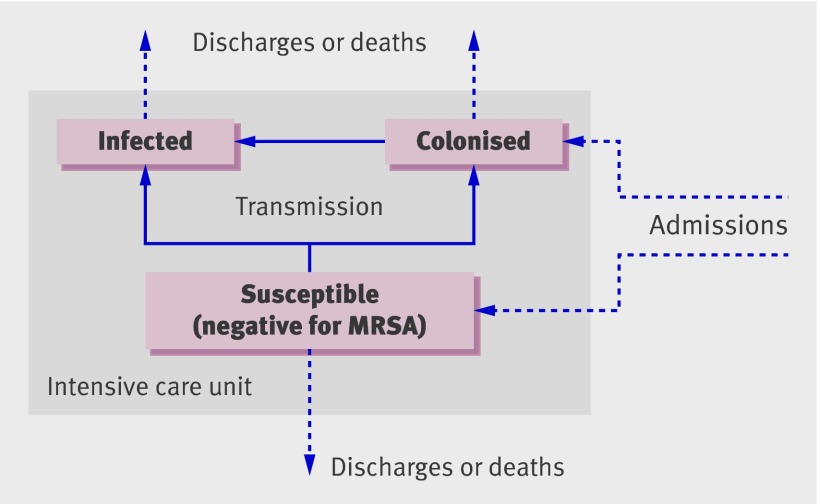
To assess the cost effectiveness of screening, isolation, and decolonisation strategies in the control of meticillin resistant Staphylococcus aureus (MRSA) in intensive care units.
Economic evaluation based on a dynamic transmission model.
England and Wales. Population Theoretical population of patients on an intensive care unit.
Infections, deaths, costs, quality adjusted life years (QALYs), incremental cost effectiveness ratios for alternative strategies, and net monetary benefits.
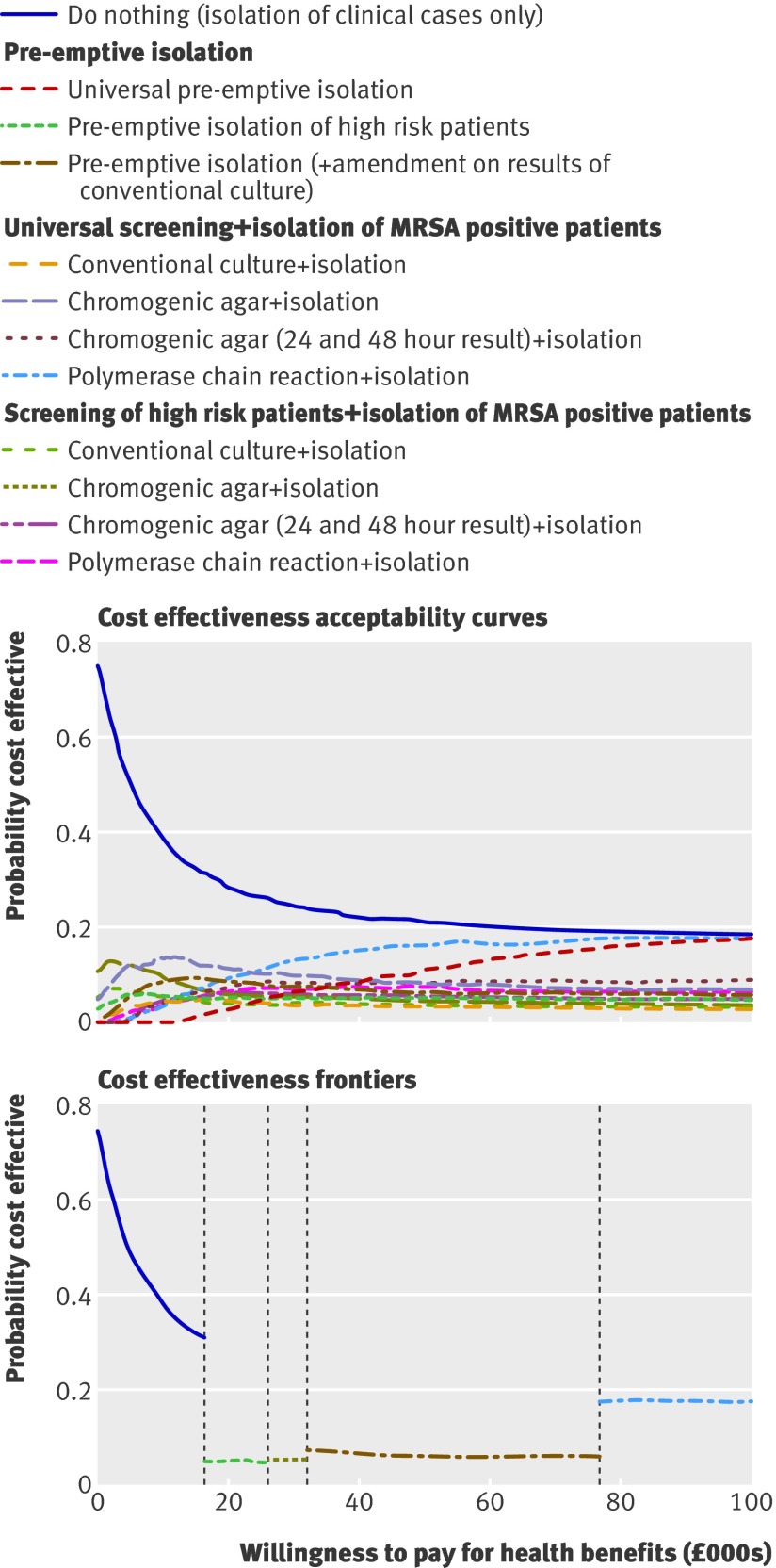
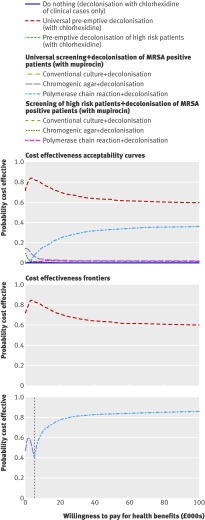
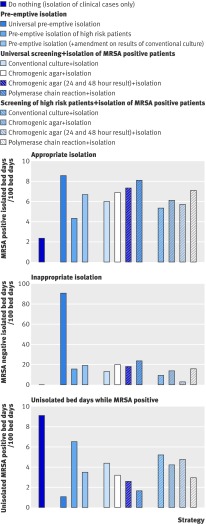
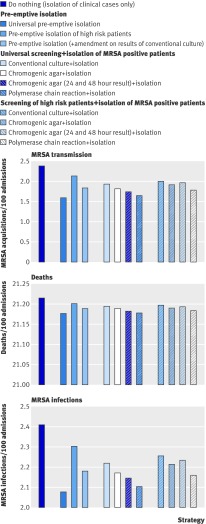
All decolonisation strategies improved health outcomes and reduced costs. Although universal decolonisation (regardless of MRSA status) was the most cost effective in the short term, strategies using screening to target MRSA carriers may be preferred owing to the reduced risk of selecting for resistance. Among such targeted strategies, universal admission and weekly screening with polymerase chain reaction coupled with decolonisation using nasal mupirocin was the most cost effective. This finding was robust to the size of intensive care units, prevalence of MRSA on admission, proportion of patients classified as high risk, and precise value of willingness to pay for health benefits. All strategies using isolation but not decolonisation improved health outcomes but costs were increased. When the prevalence of MRSA on admission to the intensive care unit was 5% and the willingness to pay per QALY gained was between £20,000 (€23,000; $32,000) and £30,000, the best such strategy was to isolate only those patients at high risk of carrying MRSA (either pre-emptively or after identification by admission and weekly screening for MRSA using chromogenic agar). Universal admission and weekly screening using polymerase chain reaction based detection of MRSA coupled with isolation was unlikely to be cost effective unless prevalence was high (10% of patients colonised with MRSA on admission).
MRSA control strategies that use decolonisation are likely to be cost saving in an intensive care unit setting provided resistance is lacking, and combining universal screening using polymerase chain reaction with decolonisation is likely to represent good value for money if untargeted decolonisation is considered unacceptable. In intensive care units where decolonisation is not implemented, evidence is insufficient to support universal screening for MRSA outside high prevalence settings.
评估在重症监护病房中,通过筛查、隔离和去定植策略控制耐甲氧西林金黄色葡萄球菌(MRSA)的成本效益。
基于动态传播模型的经济评估。
英格兰和威尔士。人口理论上 ICU 患者的人群。
感染、死亡、成本、质量调整生命年(QALY)、替代策略的增量成本效益比以及净货币收益。
所有去定植策略均改善了健康结局并降低了成本。虽然无论 MRSA 状态如何,普遍去定植(universal decolonisation)都是短期最具成本效益的,但由于选择耐药的风险降低,使用筛查来针对 MRSA 携带者的策略可能更受欢迎。在这些有针对性的策略中,普遍入院和每周使用聚合酶链反应进行筛查,结合使用莫匹罗星去定植是最具成本效益的。这一发现对于 ICU 规模、入院时 MRSA 的流行率、被归类为高风险的患者比例以及对健康获益的意愿支付价值的精确性均具有稳健性。所有使用隔离但不进行去定植的策略均改善了健康结局,但成本增加。当 ICU 入院时 MRSA 的流行率为 5%,且每获得一个 QALY 的意愿支付在 20000 英镑(23000 欧元;32000 美元)至 30000 英镑之间时,最佳策略是仅对那些具有高携带 MRSA 风险的患者进行隔离(无论是预先还是通过入院时的筛查,以及每周使用显色琼脂对 MRSA 进行筛查来确定)。只有在流行率较高(入院时 10%的患者定植有 MRSA)的情况下,普遍入院和每周使用聚合酶链反应检测 MRSA 的筛查结合隔离才可能具有成本效益。在 ICU 环境中,如果不实施去定植策略,由于缺乏耐药性,使用去定植的 MRSA 控制策略可能会节省成本,并且如果不考虑普遍去定植,那么使用聚合酶链反应进行普遍筛查加上去定植可能具有很好的性价比。在未实施去定植的 ICU 中,尚无足够证据支持在高流行率环境之外进行针对 MRSA 的普遍筛查。