School of Nursing, Faculty of Medical and Health Sciences, University of Auckland, Auckland, New Zealand.
Int J Equity Health. 2011 Oct 20;10:45. doi: 10.1186/1475-9276-10-45.
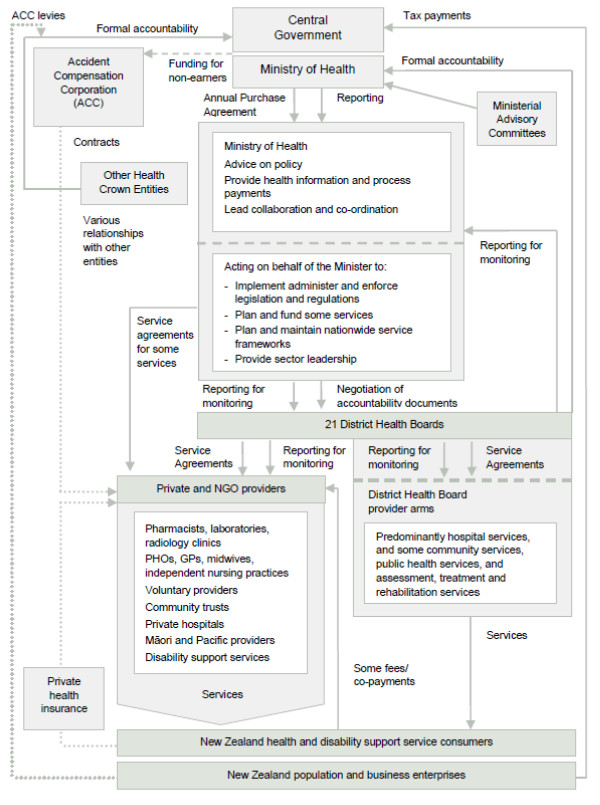
In all countries people experience different social circumstances that result in avoidable differences in health. In New Zealand, Māori, Pacific peoples, and those with lower socioeconomic status experience higher levels of chronic illness, which is the leading cause of mortality, morbidity and inequitable health outcomes. Whilst the health system can enable a fairer distribution of good health, limited national data is available to measure health equity. Therefore, we sought to find out whether health services in New Zealand were equitable by measuring the level of development of components of chronic care management systems across district health boards. Variation in provision by geography, condition or ethnicity can be interpreted as inequitable.
A national survey of district health boards (DHBs) was undertaken on macro approaches to chronic condition management with detail on cardiovascular disease, chronic obstructive pulmonary disease, congestive heart failure, stroke and diabetes. Additional data from expert informant interviews on program reach and the cultural needs of Māori and Pacific peoples was sought. Survey data were analyzed on dimensions of health equity relevant to strategic planning and program delivery. Results are presented as descriptive statistics and free text. Interviews were transcribed and NVivo 8 software supported a general inductive approach to identify common themes.
Survey responses were received from the majority of DHBs (15/21), some PHOs (21/84) and 31 expert informants. Measuring, monitoring and targeting equity is not systematically undertaken. The Health Equity Assessment Tool is used in strategic planning but not in decisions about implementing or monitoring disease programs. Variable implementation of evidence-based practices in disease management and multiple funding streams made program implementation difficult. Equity for Māori is embedded in policy, this is not so for other ethnic groups or by geography. Populations that conventional practitioners find hard to reach, despite recognized needs, are often underserved. Nurses and community health workers carried a disproportionate burden of care. Cultural and diversity training is not a condition of employment.
There is a struggle to put equity principles into practice, indicating will without enactment. Equity is not addressed systematically below strategic levels and equity does not shape funding decisions, program development, implementation and monitoring. Equity is not incentivized although examples of exceptional practice, driven by individuals, are evident across New Zealand.
在所有国家,人们都面临着不同的社会环境,这些环境导致健康方面存在不可避免的差异。在新西兰,毛利人、太平洋岛民以及社会经济地位较低的人群患慢性病的比例较高,而慢性病是导致死亡、发病和健康结果不平等的主要原因。虽然卫生系统可以实现更公平的健康分配,但衡量卫生公平性的全国性数据有限。因此,我们试图通过衡量各地区卫生局(DHB)的慢性病管理系统各组成部分的发展程度,来了解新西兰的卫生服务是否公平。地理、条件或种族的供应差异可以被解释为不公平。
对地区卫生局(DHB)进行了一项关于慢性病管理宏观方法的全国性调查,详细介绍了心血管疾病、慢性阻塞性肺疾病、充血性心力衰竭、中风和糖尿病的情况。还从专家信息员那里收集了关于项目覆盖范围以及毛利人和太平洋岛民的文化需求的额外数据。对与战略规划和项目交付相关的卫生公平维度进行了调查数据分析。结果以描述性统计和自由文本呈现。采访记录被转录,使用 NVivo 8 软件支持采用一般归纳法识别共同主题。
收到了来自大多数 DHB(15/21)、一些 PHO(21/84)和 31 位专家信息员的调查回复。衡量、监测和针对公平性进行目标定位没有系统地进行。卫生公平评估工具用于战略规划,但不用于决定实施或监测疾病项目。疾病管理中基于证据的实践的实施情况存在差异,并且存在多个资金来源,这使得项目实施变得困难。毛利人的公平性嵌入在政策中,而其他族裔群体或地理因素则不然。尽管存在公认的需求,但传统医生难以接触到的人群往往服务不足。护士和社区卫生工作者承担了不成比例的护理负担。文化和多样性培训不是就业的条件。
在实践中实施公平原则存在困难,表明有意愿但无行动。公平性没有在战略层面以下得到系统解决,公平性也没有影响资金决策、项目开发、实施和监测。虽然新西兰各地都有个人驱动的卓越实践的例子,但没有激励公平性。