Centre for Health Service Development, Building 234, iC Enterprise 1, Innovation Campus, University of Wollongong, NSW 2522, Australia.
BMC Health Serv Res. 2011 Oct 31;11:291. doi: 10.1186/1472-6963-11-291.
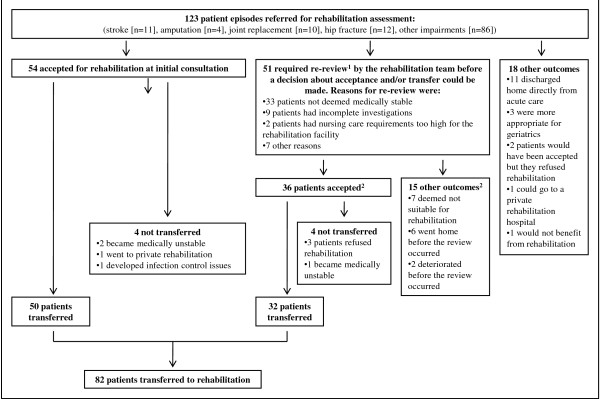
The selection of patients for rehabilitation, and the timing of transfer from acute care, are important clinical decisions that impact on care quality and patient flow. This paper reports utilization review data on inpatients in acute care with stroke, hip fracture or elective joint replacement, and other inpatients referred for rehabilitation. It examines reasons why acute level of care criteria are not met and explores differences in decision making between acute care and rehabilitation teams around patient appropriateness and readiness for transfer.
Cohort study of patients in a large acute referral hospital in Australia followed with the InterQual utilization review tool, modified to also include reasons why utilization criteria are not met. Additional data on team decision making about appropriateness for rehabilitation, and readiness for transfer, were collected on a subset of patients.
There were 696 episodes of care (7189 bed days). Days meeting acute level of care criteria were 56% (stroke, hip fracture and joint replacement patients) and 33% (other patients, from the time of referral). Most inappropriate days in acute care were due to delays in processes/scheduling (45%) or being more appropriate for rehabilitation or lower level of care (30%).On the subset of patients, the acute care team and the utilization review tool deemed patients ready for rehabilitation transfer earlier than the rehabilitation team (means of 1.4, 1.3 and 4.0 days from the date of referral, respectively). From when deemed medically stable for transfer by the acute care team, 28% of patients became unstable. From when deemed stable by the rehabilitation team or utilization review, 9% and 11%, respectively, became unstable.
A high proportion of patient days did not meet acute level of care criteria, due predominantly to inefficiencies in care processes, or to patients being more appropriate for an alternative level of care, including rehabilitation. The rehabilitation team was the most accurate in determining ongoing medical stability, but at the cost of a longer acute stay.To avoid inpatients remaining in acute care in a state of 'terra nullius', clinical models which provide rehabilitation within acute care, and more efficient movement to a rehabilitation setting, is required. Utilization review could have a decision support role in the determination of medical stability.
患者的康复选择以及从急性护理转移的时机是影响护理质量和患者流程的重要临床决策。本文报告了对急性护理中患有中风、髋部骨折或择期关节置换的住院患者以及转往康复科的其他住院患者进行利用审查的数据。它检查了不符合急性护理标准的原因,并探讨了急性护理和康复团队在患者是否适合和准备转往康复科方面的决策差异。
对澳大利亚一家大型急性转诊医院的患者进行队列研究,使用 InterQual 利用审查工具进行跟踪,该工具已修改为还包括不符合利用标准的原因。对一部分患者还收集了关于团队对康复适宜性和转往康复科准备情况的决策的额外数据。
共有 696 次护理(7189 个床位日)。符合急性护理标准的天数为 56%(中风、髋部骨折和关节置换患者)和 33%(其他患者,从转往康复科的时间开始)。急性护理中大多数不适当的天数是由于流程/计划延迟(45%)或更适合康复或更低级别的护理(30%)造成的。在亚组患者中,急性护理团队和利用审查工具认为患者准备好进行康复转科的时间早于康复团队(从转往康复科的日期开始分别为 1.4、1.3 和 4.0 天)。从急性护理团队认为患者适合转科的那一刻起,28%的患者变得不稳定。从康复团队或利用审查认为患者稳定的那一刻起,分别有 9%和 11%的患者变得不稳定。
相当多的患者住院天数不符合急性护理标准,主要是由于护理流程效率低下,或者患者更适合替代级别的护理,包括康复。康复团队最准确地确定了持续的医学稳定性,但代价是急性住院时间延长。为了避免患者在急性护理中处于“无主之地”的状态,需要提供急性护理内康复的临床模式,并更有效地转往康复环境。利用审查可以在确定医学稳定性方面发挥决策支持作用。