Division of Health Services Policy and Practice, Department of Epidemiology and Environmental Health, University at Buffalo, Buffalo, New York.
Department of Rehabilitation Science, University at Buffalo, Buffalo, New York.
JAMA Netw Open. 2020 Mar 2;3(3):e201204. doi: 10.1001/jamanetworkopen.2020.1204.
Enrollment in Medicare Advantage (MA) has been increasing and has reached one-third of total Medicare enrollment. Because of data limitations, direct comparison of inpatient rehabilitation services between MA and traditional Medicare (TM) beneficiaries has been very scarce. Subgroups of elderly individuals admitted to inpatient rehabilitation facilities (IRFs) may experience different care outcomes by insurance types.
To measure the differences in length of stay and health outcomes of inpatient rehabilitation services between TM and MA beneficiaries in the US.
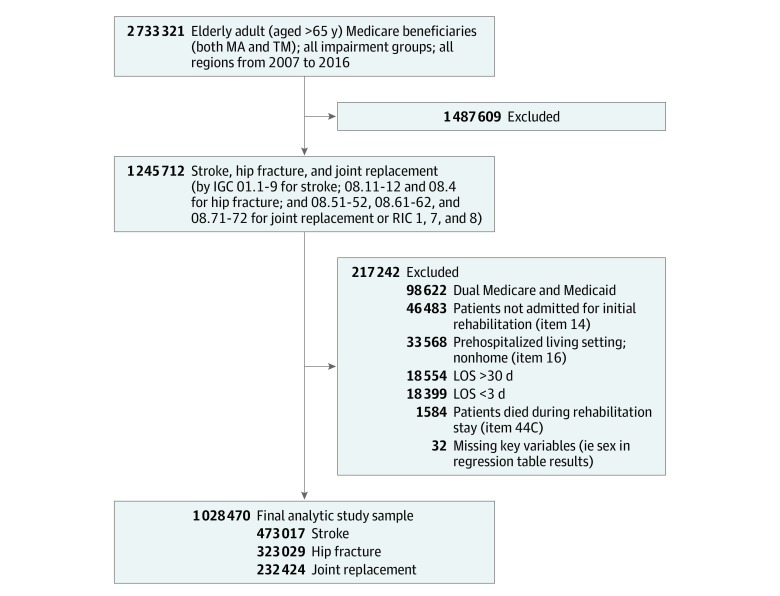
DESIGN, SETTING, AND PARTICIPANTS: This multiyear cross-sectional study used the Uniform Data System for Medical Rehabilitation to assess rehabilitation services received by elderly (aged >65 years) Medicare beneficiaries in IRFs between 2007 and 2016 for stroke, hip fracture, and joint replacement. Generalized linear models were used to assess whether an association existed between Medicare insurance type and IRF care outcomes. Models were adjusted for demographic characteristics, clinical conditions, and facility characteristics. Data were analyzed from September 2018 to August 2019.
Medicare insurance plan type, TM or MA.
Inpatient length of stay in IRFs, functional improvements, and possibility of returning to the community after discharge.
The sample included a total of 1 028 470 patients (634 619 women [61.7%]; mean [SD] age, 78.23 [7.26] years): 473 017 patients admitted for stroke, 323 029 patients admitted for hip fracture, and 232 424 patients admitted for joint replacement. Individuals enrolled in MA plans were younger than TM beneficiaries (mean [SD] age, 76.96 [7.02] vs 77.95 [7.26] years for stroke, 79.92 [6.93] vs 80.85 [6.87] years for hip fracture, and 74.79 [6.58] vs 75.88 [6.80] years for joint replacement) and were more likely to be black (17 086 [25.5%] vs 54 648 [17.9%] beneficiaries) or Hispanic (14 496 [28.5%] vs 24 377 [8.3%] beneficiaries). The MA beneficiaries accounted for 21.8% (103 204 of 473 017) of admissions for stroke, 11.5% (37 160 of 323 029) of admissions for hip fracture, and 11.8% (27 314 of 232 424) of admissions for joint replacement. The MA beneficiaries had shorter mean lengths of stay than did TM beneficiaries for both stroke (0.11 day; 95% CI, -0.15 to -0.07 day; 1.15% shorter) and hip fracture (0.17 day; 95% CI, -0.21 to -0.13 day; 0.85% shorter). The MA beneficiaries also had higher possibilities of returning to the community than did TM beneficiaries, by 3.0% (95% CI, 2.6%-3.4%) for stroke and 5.0% (95% CI, 4.4%-5.6%) for hip fracture. The shorter length of stay and better ultimate outcomes were achieved without substantially compromising the intermediate functional improvements. Facility type (freestanding vs within an acute care hospital) and patient alternative payment sources other than Medicare (none vs other) partially explained the differences between insurance types.
This study suggests that MA enrollees experience shorter length of stay and better outcomes for postacute care than do TM beneficiaries in IRFs. The magnitude of the differences depends on treatment deferability, patient sociodemographic subgroups, and facility characteristics.
医疗保险优势(MA)的参保人数一直在增加,现已达到医疗保险参保总人数的三分之一。由于数据限制,MA 和传统医疗保险(TM)受益人的住院康复服务直接比较非常有限。入住住院康复机构(IRF)的老年个体亚组可能因保险类型的不同而经历不同的护理结果。
测量美国 TM 和 MA 受益人在住院康复服务方面的住院时间和健康结果的差异。
设计、地点和参与者:这项多年的横断面研究使用统一数据系统对医疗康复,评估了 2007 年至 2016 年间 IRF 中年龄(>65 岁)的 Medicare 受益人的康复服务,这些受益人的疾病包括中风、髋部骨折和关节置换。使用广义线性模型评估医疗保险类型与 IRF 护理结果之间是否存在关联。模型根据人口统计学特征、临床状况和设施特征进行了调整。数据分析于 2018 年 9 月至 2019 年 8 月进行。
医疗保险计划类型,TM 或 MA。
IRF 的住院时间、功能改善以及出院后返回社区的可能性。
样本共包括 1028470 名患者(634619 名女性[61.7%];平均[标准差]年龄,78.23[7.26]岁):473017 名患者因中风入院,323029 名患者因髋部骨折入院,232424 名患者因关节置换入院。参加 MA 计划的患者比 TM 受益人的年龄更小(平均[标准差]年龄,中风为 76.96[7.02]岁 vs 77.95[7.26]岁,髋部骨折为 79.92[6.93]岁 vs 80.85[6.87]岁,关节置换为 74.79[6.58]岁 vs 75.88[6.80]岁),并且更有可能是黑人(17086[25.5%] vs 54648[17.9%]名受益人)或西班牙裔(14496[28.5%] vs 24377[8.3%]名受益人)。MA 受益人的住院人数占中风(473017 名)的 21.8%(103204 名),髋部骨折(323029 名)的 11.5%(37160 名)和关节置换(232424 名)的 11.8%(27314 名)。MA 受益人的平均住院时间比 TM 受益人的平均住院时间短,中风为 0.11 天(95%置信区间[CI],-0.15 至-0.07 天;1.15%更短),髋部骨折为 0.17 天(95% CI,-0.21 至-0.13 天;0.85%更短)。MA 受益人的出院后返回社区的可能性也比 TM 受益人的可能性更高,中风为 3.0%(95% CI,2.6%-3.4%),髋部骨折为 5.0%(95% CI,4.4%-5.6%)。在不明显影响中期功能改善的情况下,实现了较短的住院时间和更好的最终结果。设施类型(独立机构与急性护理医院内)和 Medicare 以外的其他患者支付来源(无与其他)部分解释了保险类型之间的差异。
这项研究表明,与 TM 受益人相比,MA 参保人在 IRF 接受康复服务的时间更短,出院后康复效果更好。差异的幅度取决于治疗的可延迟性、患者的社会人口统计学亚组和设施特征。