Müller Andreas
Department of Otorhinolaryngology/Plastic Surgery, SRH Wald-Klinikum Gera gGmbH, teaching hospital of the Friedrich-Schiller-University Jena, Gera.
GMS Curr Top Otorhinolaryngol Head Neck Surg. 2005;4:Doc09. Epub 2005 Sep 28.
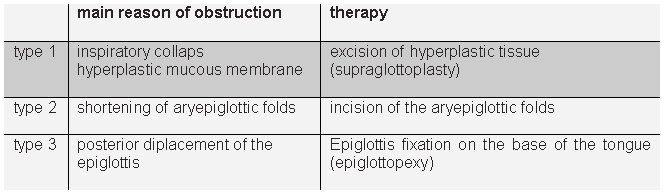
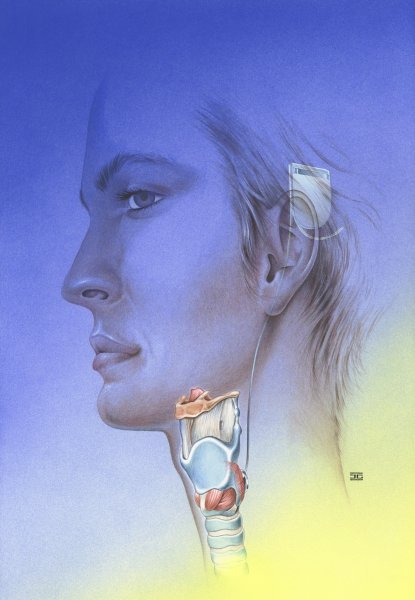
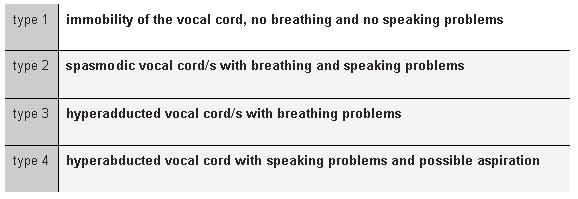
The larynx is the "bottleneck" of the human airway. For this reason, the effects of stenosing laryngeal pathologies on the vital factor respiratory gas exchange are particularly critical.Internal stabilization is a prerequisite for recovery of the laryngeal respiratory function in severe forms of inspiratory collapse (laryngomalacia). Effective laser surgery techniques have been developed to this end in recent years.Glottis-dilating surgery in cases of bilateral vocal cord motion impairment is now moving in the direction of endoscopic laser cordotomy or cordectomy, whereas arytenoidectomy and open surgical procedures are now used only rarely due to higher secondary morbidity rates. In individual cases, in particular if functional recovery is expected, temporary laterofixation of a vocal cord using an endoscopic suturing technique can be a helpful approach.Extensive laryngeal defects can be covered by means of composite grafts with mucosal lining, a supporting skeleton and their own vascularization. Autologous transplantation of the larynx, with its complex surgical and immunological problems, has become a manageable procedure. The problems of post-transplantation reinnervation and risk assessment of immunosuppression-induced recurrence of the tumor are still under consideration.Reanimation of the bilaterally paralyzed larynx by means of neurorrhaphy (neurosuture), neural grafting and, more recently, functional electrostimulation (pacemaker) represents a challenge for the coming years. In most cases of paralysis of the recurrent laryngeal nerve, a part of the muscles is maintained by synkinetic reinnervation when therapy is carried out, which however also prevents effective vocal cord movement due to simultaneous activity of agonists and antagonists. Modulation of reinnervation by means of electrostimulation and modern genetic therapy approaches justify hopes of better outcomes in the future.
喉是人类气道的“瓶颈”。因此,喉狭窄性病变对关键因素呼吸气体交换的影响尤为关键。对于严重形式的吸气性塌陷(喉软化症),内部稳定是恢复喉呼吸功能的前提条件。近年来已为此开发了有效的激光手术技术。对于双侧声带运动障碍的病例,声门扩张手术目前正朝着内镜激光声带切开术或声带切除术的方向发展,而由于较高的继发性发病率,杓状软骨切除术和开放手术目前很少使用。在个别情况下,特别是如果预期功能恢复,使用内镜缝合技术临时将声带侧向固定可能是一种有用的方法。广泛的喉部缺损可以通过带有黏膜衬里、支撑骨架及其自身血管化的复合移植物来覆盖。喉的自体移植,尽管存在复杂的手术和免疫学问题,但已成为一种可操作的手术。移植后再支配问题以及免疫抑制引起肿瘤复发的风险评估仍在研究中。通过神经缝合(神经缝线)、神经移植以及最近的功能性电刺激(起搏器)使双侧麻痹的喉恢复功能,是未来几年的一项挑战。在大多数喉返神经麻痹的病例中,在进行治疗时,一部分肌肉通过联带运动再支配得以保留,但这也由于激动剂和拮抗剂的同时活动而妨碍了有效的声带运动。通过电刺激和现代基因治疗方法调节再支配,为未来取得更好的结果带来了希望。