Pismensky Sergei V, Kalzhanov Zhomart R, Eliseeva Marina Yu, Kosmas Ioannis P, Mynbaev Ospan A
Laboratory of Pathophysiology, Faculty of Basic Medicine, M.V. Lomonosov Moscow State University, Lomonosovsky Prospekt 31-5, Moscow, 117192, Russia.
BMC Surg. 2011 Nov 14;11:30. doi: 10.1186/1471-2482-11-30.
Many factors have been put forward as a driving mechanism of surgery-triggered adhesion formation (AF). In this study, we underline the key role of specific surgical trauma related with open surgery (OS) and laparoscopic (LS) conditions in postoperative AF and we aimed to study peritoneal tissue inflammatory reaction (TIR), remodelling specific complications of open surgery (OS) versus LS and subsequently evaluating AF induced by these conditions.
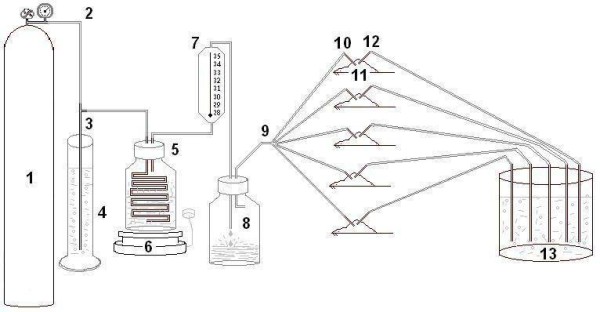
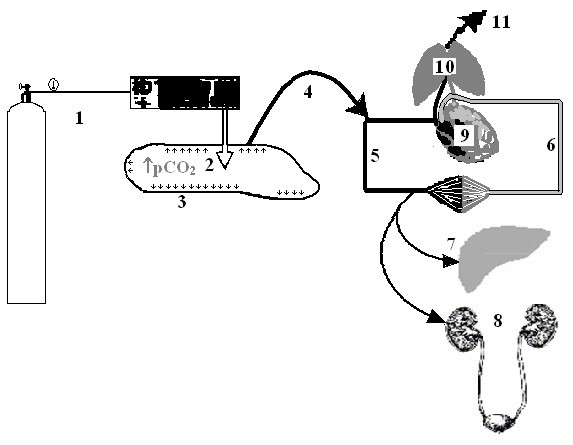
A prospective randomized study was done in 80 anaesthetised female Wistar rats divided equally into 2 groups. Specific traumatic OS conditions were induced by midline incision line (MIL) extension and tissue drying and specific LS conditions were remodelled by intraperitoneal CO2 insufflation at the 10 cm of water. TIR was evaluated at the 24th, 72nd, 120th and 168th hour by scoring scale. Statistical analysis was performed by the non-parametric t test and two-way ANOVA using Bonferroni post-tests.
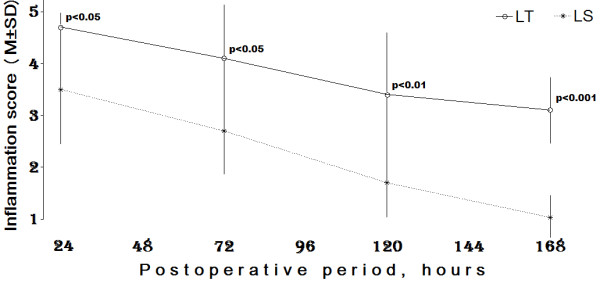
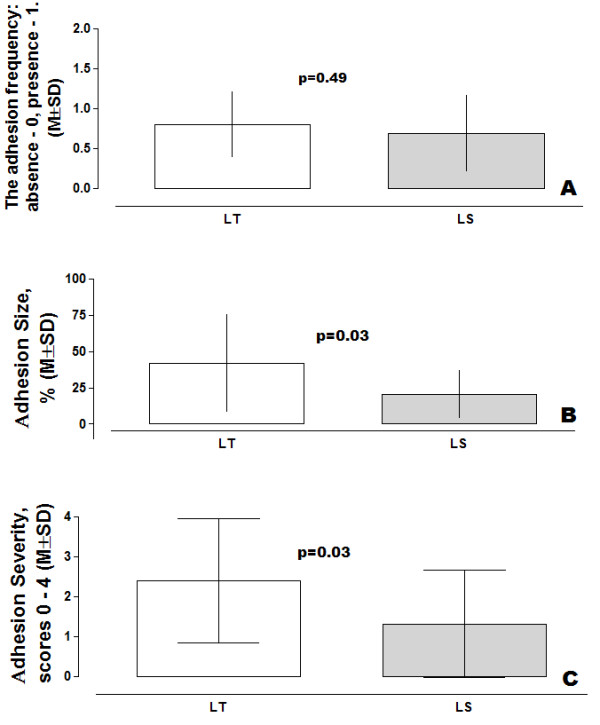
More pronounced residual TIR was registered after OS than after LS. There were no significant TIR interactions though highly significant differences were observed between the OS and LS groups (p < 0.0001) with regard to surgical and time factors. The TIR change differences between the OS and LS groups were pronounced with postoperative time p < 0.05 at the 24th and 72nd; p < 0.01--120th and p < 0.001--168th hrs. Adhesion free wounds were observed in 20.0 and 31.0% of cases after creation of OS and LS conditions respectively; with no significant differences between these values (p > 0.05). However larger adhesion size (41.67 ± 33.63) was observed after OS in comparison with LS (20.31 ± 16.38). The upper-lower 95% confidential limits ranged from 60.29 to 23.04 and from 29.04 to 11.59 respectively after OS and LS groups with significant differences (p = 0.03). Analogous changes were observed in adhesion severity values. Subsequently, severe TIR parameters were followed by larger sizes of severe postoperative adhesions in the OS group than those observed in the LS group.
MIL extension and tissue drying seem to be the key factors in the pathogenesis of adhesion formation, triggering severe inflammatory reactions of the peritoneal tissue surrounding the MIL resulting in local and systemic consequences. CO2 insufflation however, led to moderate inflammation and less adhesion formation.
许多因素被提出作为手术引发粘连形成(AF)的驱动机制。在本研究中,我们强调了与开放手术(OS)和腹腔镜手术(LS)相关的特定手术创伤在术后AF中的关键作用,并且我们旨在研究腹膜组织炎症反应(TIR)、开放手术(OS)与腹腔镜手术(LS)的重塑特定并发症,随后评估由这些情况诱导的AF。
对80只麻醉的雌性Wistar大鼠进行前瞻性随机研究,将其平均分为2组。通过中线切口延长(MIL)和组织干燥诱导特定的创伤性OS情况,通过在10厘米水柱压力下进行腹腔内二氧化碳充气来重塑特定的LS情况。在第24、72、120和168小时通过评分量表评估TIR。使用Bonferroni事后检验,通过非参数t检验和双向方差分析进行统计分析。
与LS后相比,OS后记录到更明显的残余TIR。尽管在手术和时间因素方面,OS组和LS组之间观察到高度显著差异(p < 0.0001),但没有显著的TIR相互作用。OS组和LS组之间的TIR变化差异在术后时间上很明显,在第24和72小时p < 0.05;在第120小时p < 0.01,在第168小时p < 0.001。在创建OS和LS情况后,分别有20.0%和31.0%的病例观察到无粘连伤口;这些值之间没有显著差异(p > 0.05)。然而,与LS(20.31 ± 16.38)相比,OS后观察到更大的粘连尺寸(41.67 ± 33.63)。OS组和LS组的上下95%置信限分别为60.29至23.04和29.04至11.59,存在显著差异(p = 0.03)。在粘连严重程度值方面观察到类似变化。随后,OS组中严重的TIR参数之后是比LS组中观察到的更大尺寸的严重术后粘连。
MIL延长和组织干燥似乎是粘连形成发病机制中的关键因素,引发围绕MIL的腹膜组织的严重炎症反应,导致局部和全身后果。然而,二氧化碳充气导致中度炎症和较少的粘连形成。