Department of Pathology, Division of Diagnostics and Intervention, Oslo University Hospital HF, Montebello, Norway.
Mod Pathol. 2012 Apr;25(4):537-47. doi: 10.1038/modpathol.2011.188. Epub 2011 Dec 9.
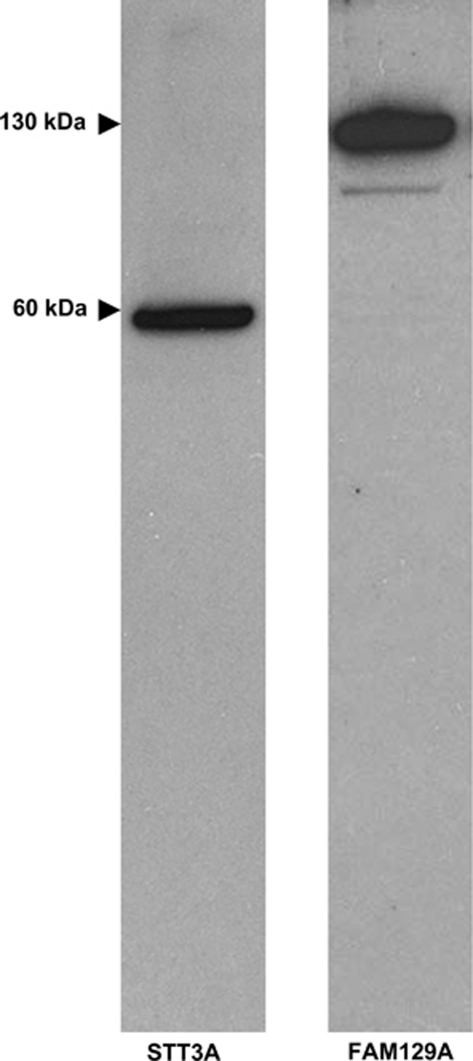
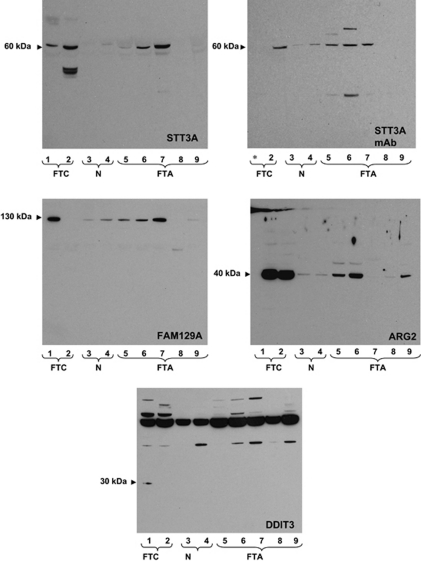
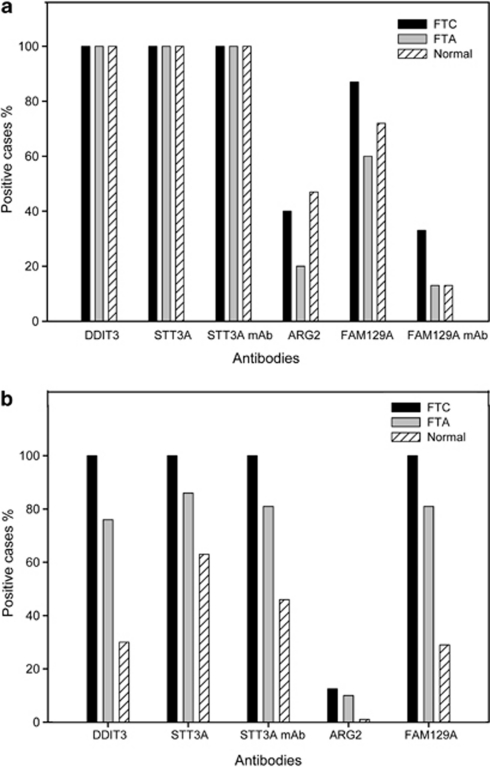
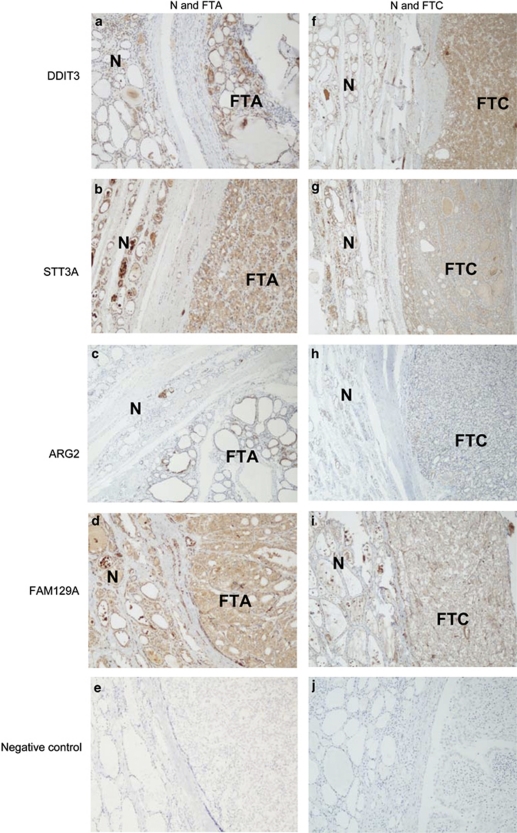
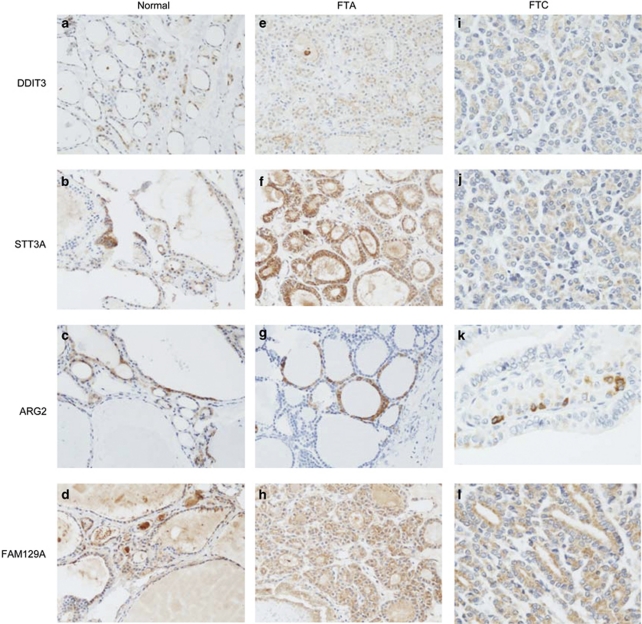
Preoperative characterization of thyroid follicular lesions is challenging. Fine-needle aspiration specimens cannot differentiate follicular carcinomas from benign follicular neoplasias. Recently, promising markers have been detected using modern molecular techniques. We conducted a retrospective study to confirm the usefulness of immunohistochemical staining for the protein markers, DDIT3, STT3A (ITM1), ARG2 and FAM129A (C1orf24) in separating benign and malignant thyroid follicular lesions. Formalin-fixed, paraffin-embedded thyroid tissue from 30 in-house cases (15 follicular carcinomas and 15 follicular adenomas), as well as 8 follicular carcinomas and 21 follicular adenomas on tissue microarray slides were stained immunohistochemically for DDIT3, STT3A, ARG2 and FAM129A expression. Control tissue consisted of thyroid parenchyma adjacent to the tumors and 11 separate cases of normal thyroid parenchyma. All in-house cases of follicular adenomas, follicular carcinomas and adjacent normal thyroid tissue showed positive immunostaining with anti-DDIT3 and anti-STT3A. Anti-ARG2 and anti-FAM129A polyclonal antibodies showed positive staining in 20 and 60% of in-house follicular adenomas, and 40 and 87% of in-house follicular carcinomas, respectively. Monoclonal anti-FAM129A demonstrated positive staining in 13 and 33% of in-house follicular adenomas and follicular carcinomas, respectively. Polyclonal anti-DDIT3, -STT3A and -FAM129A antibodies showed positive staining in all tissue microarray slides of follicular carcinoma and in 76, 85 and 81% of the follicular adenomas, respectively. Monoclonal anti-STT3A stained 81% of the follicular adenoma cores. Anti-ARG2 stained positive in 13% of follicular carcinomas and 10% of follicular adenomas on the tissue microarray slides. In conclusion, DDIT3, STT3A, ARG2 and FAM129A immunohistochemistry does not appear to be useful in the diagnosis of thyroid follicular neoplasias, as they do not reliably distinguish follicular thyroid carcinoma from follicular thyroid adenoma.
术前甲状腺滤泡性病变的特征具有挑战性。细针穿刺标本不能将滤泡癌与良性滤泡性肿瘤区分开来。最近,使用现代分子技术检测到了有前途的标记物。我们进行了一项回顾性研究,以确认免疫组织化学染色对蛋白标记物 DDIT3、STT3A(ITM1)、ARG2 和 FAM129A(C1orf24)在区分良性和恶性甲状腺滤泡性病变中的有用性。使用福尔马林固定、石蜡包埋的甲状腺组织,对 30 例院内病例(15 例滤泡癌和 15 例滤泡性腺瘤)以及组织微阵列载玻片上的 8 例滤泡癌和 21 例滤泡性腺瘤进行 DDIT3、STT3A、ARG2 和 FAM129A 表达的免疫组织化学染色。对照组织包括肿瘤旁甲状腺实质和 11 例单独的正常甲状腺实质。所有院内滤泡性腺瘤、滤泡癌和相邻正常甲状腺组织均对抗 DDIT3 和抗 STT3A 免疫染色呈阳性。抗 ARG2 和抗 FAM129A 多克隆抗体在 20%和 60%的院内滤泡性腺瘤和 40%和 87%的院内滤泡癌中显示阳性染色。单克隆抗 FAM129A 在 13%和 33%的院内滤泡性腺瘤和滤泡癌中显示阳性染色。多克隆抗 DDIT3、STT3A 和抗 FAM129A 抗体在所有组织微阵列载玻片的滤泡癌中均呈阳性染色,在 76%、85%和 81%的滤泡性腺瘤中分别呈阳性染色。单克隆抗 STT3A 染色了 81%的滤泡性腺瘤核。抗 ARG2 在组织微阵列载玻片上的滤泡癌中阳性染色 13%,在滤泡性腺瘤中阳性染色 10%。总之,DDIT3、STT3A、ARG2 和 FAM129A 免疫组化似乎不能用于甲状腺滤泡性肿瘤的诊断,因为它们不能可靠地区分滤泡性甲状腺癌和滤泡性甲状腺腺瘤。