Department of Cardiology, Thoraxcentre, Erasmus University, Rotterdam, the Netherlands.
Neth Heart J. 2012 Jan;20(1):16-23. doi: 10.1007/s12471-011-0224-z.
To assess treatment decision and outcome in patients referred for transcatheter aortic valve implantation (TAVI) in addition to predictive factors of mortality after TAVI.
Three-centre prospective observational study including 358 patients. Endpoints were defined according to the Valve Academic Research Consortium.
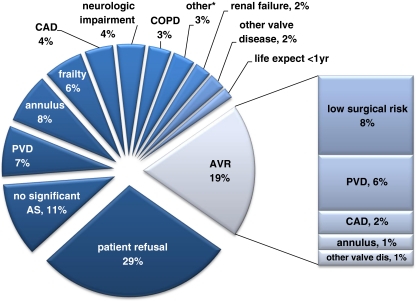
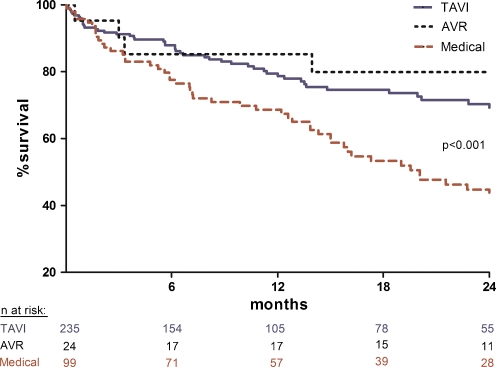
Of the 358 patients referred for TAVI, TAVI was performed in 235 patients (65%), surgical aortic valve replacement (AVR) in 24 (7%) and medical therapy (MT) in 99 (28%). Reasons to decline TAVI in favour of AVR/MT were patient preference (29%), peripheral vascular disease (15%) and non-severe aortic stenosis (11%). The logistic EuroSCORE was significantly higher in patients who underwent TAVI and MT in comparison with those undergoing AVR (19 vs. 10%, p = 0.007). At 30 days, all-cause mortality and the combined safety endpoint were 9 and 24% after TAVI and 8 and 25% after AVR, respectively. All-cause mortality was significantly lower in the TAVI group compared with the MT group at 6 months, 1 year and 2 years (12% vs. 22%, 21% vs. 33% and 31% vs. 55%, respectively, p < 0.001). Multivariable analysis revealed that blood transfusion (HR: 1.19; 95% CI: 1.05-1.33), pre-existing renal failure (HR: 1.18; 95% CI: 1.06-1.33) and STS score (HR: 1.06; 95% CI: 1.02-1.10) were independent predictors of mortality at a median of 10 (IQR: 3-23) months after TAVI.
Approximately two-thirds of the patients referred for TAVI receive this treatment with gratifying short- and long-term survival. Another 7% underwent AVR. Prognosis is poor in patients who do not receive valve replacement therapy.
评估接受经导管主动脉瓣置换术(TAVI)治疗的患者的治疗决策和结局,以及 TAVI 后死亡率的预测因素。
这是一项包括 358 名患者的三中心前瞻性观察研究。终点根据 Valve Academic Research Consortium 定义。
在 358 名被推荐接受 TAVI 的患者中,235 名(65%)接受了 TAVI,24 名(7%)接受了主动脉瓣置换术(AVR),99 名(28%)接受了药物治疗(MT)。拒绝 TAVI 而选择 AVR/MT 的原因包括患者偏好(29%)、外周血管疾病(15%)和非严重主动脉瓣狭窄(11%)。接受 TAVI 和 MT 的患者的 logistic EuroSCORE 明显高于接受 AVR 的患者(19%比 10%,p=0.007)。30 天时,TAVI 和 AVR 后全因死亡率和联合安全性终点分别为 9%和 24%,MT 后分别为 24%和 25%。TAVI 组 6 个月、1 年和 2 年时的全因死亡率明显低于 MT 组(分别为 12%比 22%、21%比 33%和 31%比 55%,p<0.001)。多变量分析显示,输血(HR:1.19;95%CI:1.05-1.33)、术前肾功能衰竭(HR:1.18;95%CI:1.06-1.33)和 STS 评分(HR:1.06;95%CI:1.02-1.10)是 TAVI 后中位 10 个月(IQR:3-23)时死亡率的独立预测因素。
大约三分之二的推荐接受 TAVI 的患者接受了治疗,并且取得了令人满意的短期和长期生存结果。另外 7%的患者接受了 AVR。未接受瓣膜置换治疗的患者预后较差。