London School of Hygiene and Tropical Medicine, London, UK.
Malar J. 2011 Dec 30;10:387. doi: 10.1186/1475-2875-10-387.
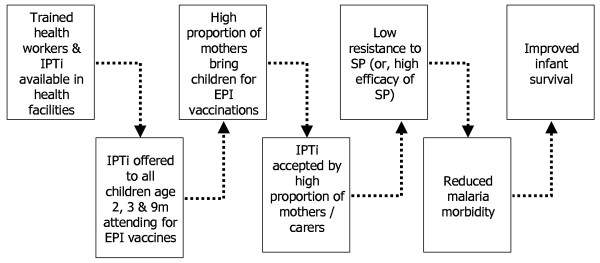
Intermittent Preventive Treatment for malaria control in infants (IPTi) consists of the administration of a treatment dose of an anti-malarial drug, usually sulphadoxine-pyrimethamine, at scheduled intervals, regardless of the presence of Plasmodium falciparum infection. A pooled analysis of individually randomized trials reported that IPTi reduced clinical episodes by 30%. This study evaluated the effect of IPTi on child survival in the context of a five-district implementation project in southern Tanzania. [
clinicaltrials.gov NCT00152204].
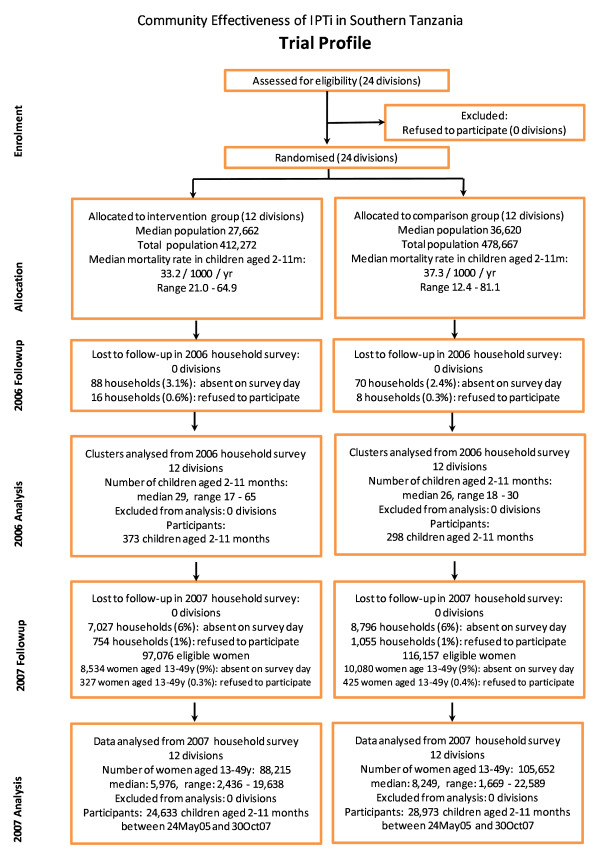
After baseline household and health facility surveys in 2004, five districts comprising 24 divisions were randomly assigned either to receive IPTi (n = 12) or not (n = 12). Implementation started in March 2005, led by routine health services with support from the research team. In 2007, a large household survey was undertaken to assess the impact of IPTi on survival in infants aged two-11 months through birth history interviews with all women aged 13-49 years. The analysis is based on an "intention-to-treat" ecological design, with survival outcomes analysed according to the cluster in which the mothers lived.
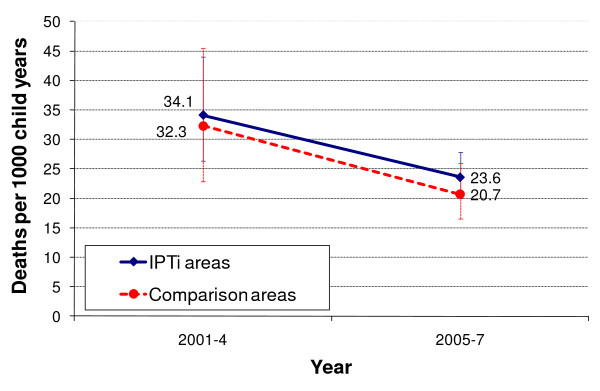
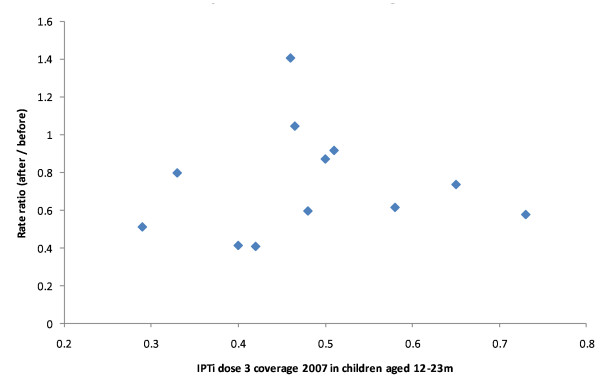
Survival in infants aged two-11 months was comparable in IPTi and comparison areas at baseline. In intervention areas in 2007, 48% of children aged 12-23 months had documented evidence of receiving three doses of IPTi, compared to 2% in comparison areas (P < 0.0001). Over the three years of the study there was a marked improvement in survival in both groups. Between 2001-4 and 2005-7, mortality rates in two-11 month olds fell from 34.1 to 23.6 per 1,000 person-years in intervention areas and from 32.3 to 20.7 in comparison areas. In 2007, divisions implementing IPTi had a 14% (95% CI -12%, 49%) higher mortality rate in two-11 month olds in comparison with non-implementing divisions (P = 0.31).
The lack of evidence of an effect of IPTi on survival could be a false negative result due to a lack of power or imbalance of unmeasured confounders. Alternatively, there could be no mortality impact of IPTi due to low coverage, late administration, drug resistance, decreased malaria transmission or improvements in vector control and case management. This study raises important questions for programme evaluation design.
间歇性预防治疗(IPT)用于控制疟疾,指的是在既定间隔时间内,为婴儿使用一剂抗疟药物(通常为磺胺多辛-乙胺嘧啶),而不论是否存在恶性疟原虫感染。个别随机试验的汇总分析报告称,IPT 可将临床发病减少 30%。本研究在坦桑尼亚南部的一个 5 区实施项目中,评估了 IPT 对儿童生存的影响。[
clinicaltrials.gov NCT00152204]。
2004 年进行基线家庭和卫生机构调查后,随机将包括 24 个分区的 5 个区分配至接受 IPT(n = 12)或不接受 IPT(n = 12)。2005 年 3 月,在研究团队的支持下,常规卫生服务启动了实施工作。2007 年,开展了一项大规模的家庭调查,通过对所有 13-49 岁妇女进行出生史访谈,评估 IPT 对 2-11 月龄婴儿生存的影响。分析采用“意向治疗”的生态设计,根据母亲所在的集群分析生存结果。
在基线时,IPT 区和对照组的 2-11 月龄婴儿的生存情况相当。在 2007 年的干预区,12-23 月龄儿童中接受了 3 剂 IPT 的比例为 48%,而对照组为 2%(P < 0.0001)。在研究的三年期间,两组的生存率都显著提高。在 2001-4 年至 2005-7 年期间,干预区和对照组的 2-11 月龄婴儿死亡率分别从 34.1/1000 人年降至 23.6/1000 人年和从 32.3/1000 人年降至 20.7/1000 人年。在 2007 年,实施 IPT 的分区与未实施分区相比,2-11 月龄婴儿的死亡率高出 14%(95%CI-12%,49%)(P = 0.31)。
IPT 对生存没有影响的证据可能是由于缺乏效力或未测量混杂因素的不平衡而导致的假阴性结果。或者,IPT 可能不会降低死亡率,原因是覆盖率低、用药延迟、耐药性、疟疾传播减少或蚊虫控制和病例管理的改善。本研究为方案评估设计提出了重要问题。