NSLIJ Healthcare System, Emergency Medicine Department, New Hyde Park, New York.
West J Emerg Med. 2011 Nov;12(4):505-11. doi: 10.5811/westjem.2011.2.1963.
Identifying fever can influence management of the emergency department (ED) patient, including diagnostic testing, treatment, and disposition. We set out to determine how well oral and tympanic membrane (TM) temperatures compared with rectal measurements.
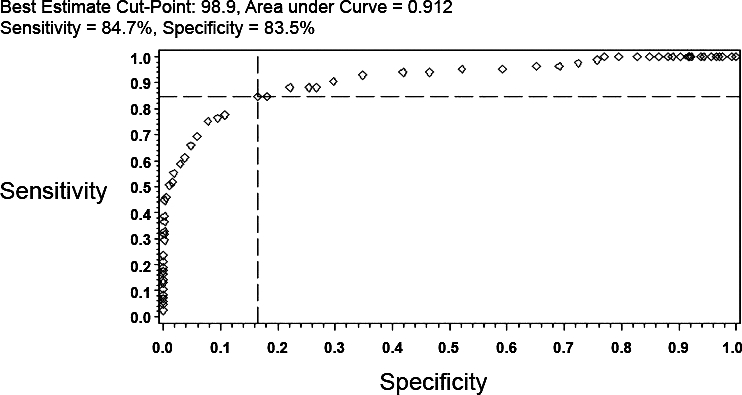
A convenience sample of consecutively adult ED patients had oral, TM, and rectal temperatures performed within several minutes of each other. Descriptive statistics, Bland-Altman agreement matrices with 95% confidence interval (CI), and measures of test performance, including sensitivity, specificity, predictive values, and interval likelihood ratios were performed.
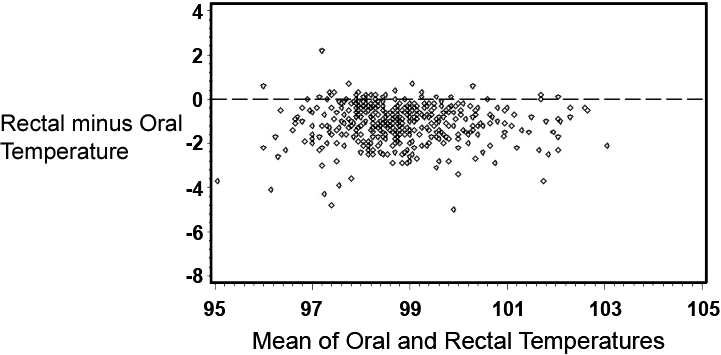
A total of 457 patients were enrolled with an average age of 64 years (standard deviation: 19 years). Mean temperatures were: oral (98.3°F), TM (99.6°F), and rectal (99.4°F). The mean difference in rectal and oral temperatures was 1.1°F, although there was considerable lack of agreement between oral and rectal temperatures, with the oral temperature as much as 2.91°F lower or 0.74°F higher than the rectal measurement (95% CI). Although the difference in mean temperature between right TM and rectal temperature was only 0.22°F, the right TM was lower than rectal by up to 1.61°F or greater by up to 2.05°F (95% CI). Test performance varied as the positive predictive value of the oral temperature was 97% and for tympanic temperature was 55% (relative to a rectal temperature of 100.4°F or higher). Comparative findings differed even at temperatures considered in the normal range; among patients with an oral temperature of 98.0 to 98.9, 38% (25/65) were found to have a rectal temperature of 100.4 or higher, while among patients with a TM of 98.0 to 98.9, only 7% (10/134) were found to have a rectal temperature of 100.4 or higher.
The oral and tympanic temperature readings are not equivalent to rectal thermometry readings. Oral thermometry frequently underestimates the temperature relative to rectal readings, and TM values can either under- or overestimate the rectal temperature. The clinician needs to be aware of the varying relationship between oral, TM, and rectal temperatures when interpreting readings.
识别发热会影响急诊科(ED)患者的处理,包括诊断性检查、治疗和处置。我们旨在确定口腔和鼓膜(TM)温度与直肠测量值相比如何。
连续对成年 ED 患者进行口腔、TM 和直肠温度测量,在数分钟内进行。进行描述性统计、95%置信区间(CI)的 Bland-Altman 一致性矩阵以及测试性能的指标,包括敏感性、特异性、预测值和间隔似然比。
共纳入 457 例患者,平均年龄为 64 岁(标准差:19 岁)。平均温度分别为:口腔(98.3°F)、TM(99.6°F)和直肠(99.4°F)。直肠和口腔温度的平均差值为 1.1°F,但口腔和直肠温度之间存在相当大的不一致,口腔温度比直肠温度低 2.91°F 或高 0.74°F(95%CI)。尽管右侧 TM 与直肠温度的平均差值仅为 0.22°F,但右侧 TM 比直肠温度低最多 1.61°F 或高最多 2.05°F(95%CI)。测试性能因口腔温度的阳性预测值为 97%,而鼓膜温度的阳性预测值为 55%(相对于直肠温度为 100.4°F 或更高)而有所不同。即使在考虑正常范围内的温度时,比较结果也存在差异;在口腔温度为 98.0 至 98.9°F 的患者中,有 38%(25/65)被发现直肠温度为 100.4°F 或更高,而在 TM 温度为 98.0 至 98.9°F 的患者中,只有 7%(10/134)被发现直肠温度为 100.4°F 或更高。
口腔和鼓膜温度读数与直肠测温读数不等效。口腔测温通常相对于直肠读数低估温度,而 TM 值可以低估或高估直肠温度。当解释读数时,临床医生需要意识到口腔、TM 和直肠温度之间的关系不同。