Unidad Clínica de Enfermedades Infecciosas, Hospitales Universitarios Virgen del Rocío/Instituto de Biomedicina de Sevilla, Seville, Spain.
PLoS One. 2012;7(1):e28115. doi: 10.1371/journal.pone.0028115. Epub 2012 Jan 3.
Data on which to base definitive recommendations on the doses and duration of therapy for genotype 3 HCV/HIV-coinfected patients are scarce. We evaluated the efficacy of a lower peginterferon-α 2a dose and a shorter duration of therapy than the current standard of care in genotype 3 HCV/HIV-coinfected patients.
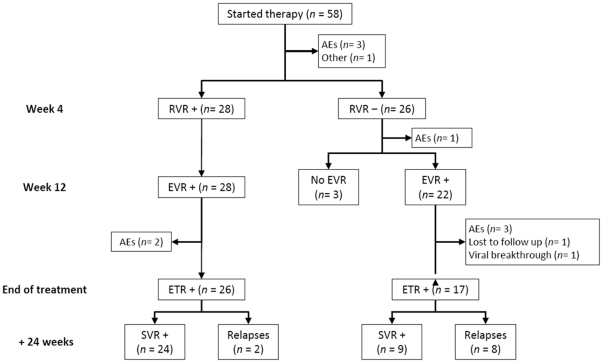
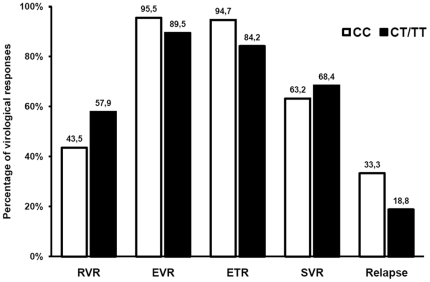
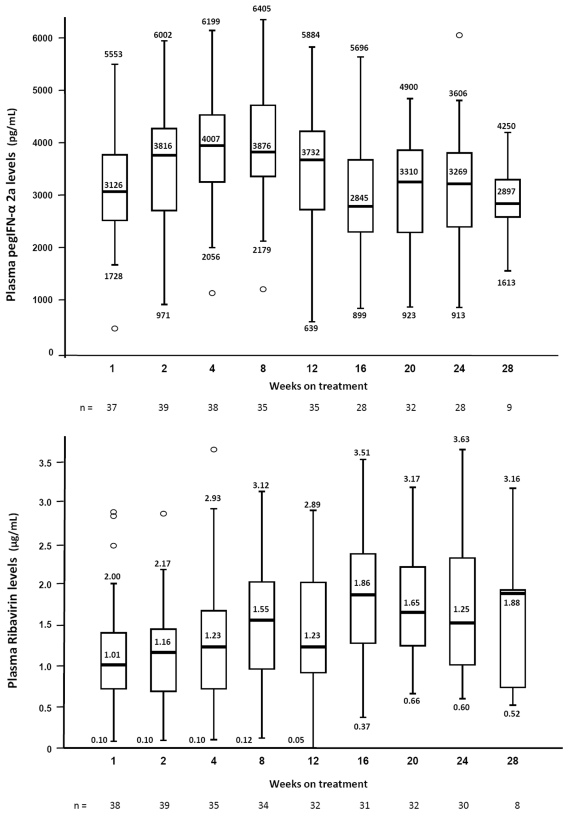
Pilot, open-label, single arm clinical trial which involved 58 Caucasian HCV/HIV-coinfected patients who received weekly 135 µg peginterferon-α 2a plus ribavirin 400 mg twice daily during 20 weeks after attaining undetectable viremia. The relationships between baseline patient-related variables, including IL28B genotype, plasma HCV-RNA, ribavirin dose/kg, peginterferon-α 2a and ribavirin levels with virological responses were analyzed. Only 4 patients showed lack of response and 5 patients dropped out due to adverse events related to the study medication. Overall, sustained virologic response (SVR) rates were 58.3% by intention-to-treat and 71.4% by per protocol analysis, respectively. Among patients with rapid virologic response (RVR), SVR and relapses rates were 92.6% and 7.4%, respectively. No relationships were observed between viral responses and ribavirin dose/kg, peginterferon-α 2a concentrations, ribavirin levels or rs129679860 genotype.
Weekly 135 µg pegIFN-α 2a could be as effective as the standard 180 µg dose, with a very low incidence of severe adverse events. A 24-week treatment duration appears to be appropriate in patients achieving RVR, but extending treatment up to just 20 weeks beyond negativization of viremia is associated with a high relapse rate in those patients not achieving RVR. There was no influence of IL28B genotype on the virological responses.
ClinicalTrials.gov NCT00553930.
目前缺乏针对基因型 3 丙型肝炎病毒/人类免疫缺陷病毒(HCV/HIV)合并感染患者的治疗剂量和疗程的明确推荐数据。我们评估了较低剂量聚乙二醇干扰素-α 2a 和较短疗程治疗基因型 3 HCV/HIV 合并感染患者的疗效,与当前的标准治疗相比。
这是一项开放性、单臂临床试验,纳入了 58 例白种人 HCV/HIV 合并感染患者,他们在达到病毒血症不可检测后,接受每周 135µg 聚乙二醇干扰素-α 2a 加利巴韦林 400mg,每日两次,共 20 周。分析了基线患者相关变量(包括 IL28B 基因型、血浆 HCV-RNA、利巴韦林剂量/kg、聚乙二醇干扰素-α 2a 和利巴韦林水平)与病毒学反应之间的关系。只有 4 例患者出现无反应,5 例患者因与研究药物相关的不良事件而退出。总的来说,意向治疗的持续病毒学应答(SVR)率分别为 58.3%和 71.4%,按方案分析。在快速病毒学应答(RVR)患者中,SVR 和复发率分别为 92.6%和 7.4%。病毒学反应与利巴韦林剂量/kg、聚乙二醇干扰素-α 2a 浓度、利巴韦林水平或 rs129679860 基因型之间无相关性。
每周 135µg 聚乙二醇干扰素-α 2a 与标准剂量 180µg 一样有效,且严重不良事件发生率极低。在达到 RVR 的患者中,24 周的治疗时间似乎是合适的,但在未达到 RVR 的患者中,将病毒血症转阴后再延长 20 周的治疗时间,会导致复发率较高。IL28B 基因型对病毒学反应没有影响。
ClinicalTrials.gov NCT00553930。